Downloaded 937 times

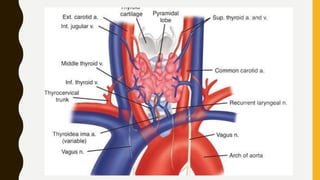

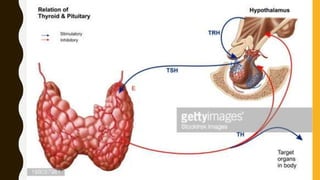
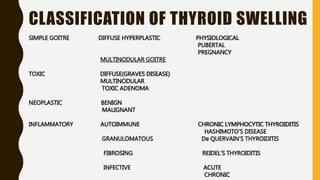
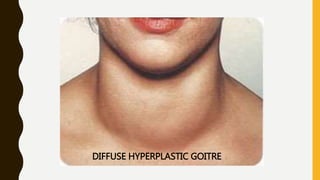
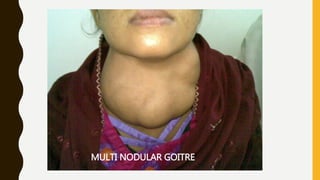


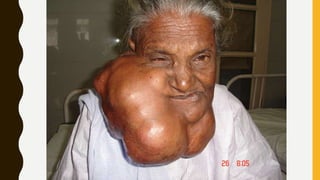



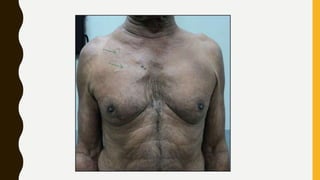
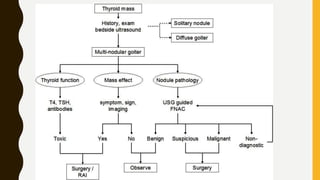

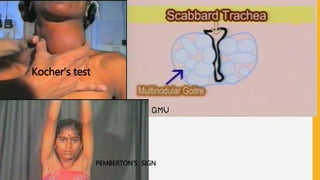


The document provides a comprehensive overview of multi-nodular goitre, covering its anatomy, classification, aetiopathogenesis, clinical features, diagnosis, treatment, and examination techniques. It explains that multi-nodular goitre can be toxic or nontoxic, with various factors contributing to its development, including iodine deficiency and goitrogens. Treatment options vary, with surgery indicated in certain cases, while prevention strategies emphasize the use of iodized salt and managing goitrogen exposure.















































![THYROID_GLAND[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidgland1-231005071359-bdb08841-thumbnail.jpg?width=640&height=640&fit=bounds)































