Downloaded 270 times


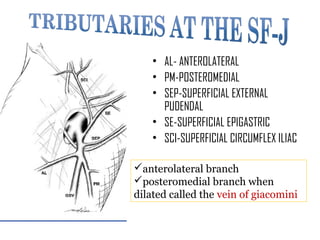
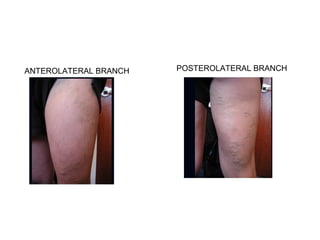

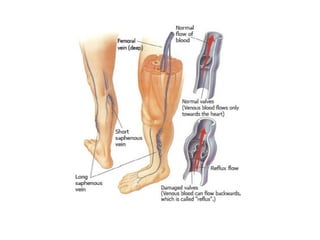
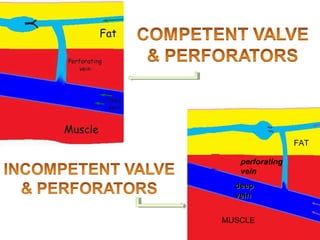
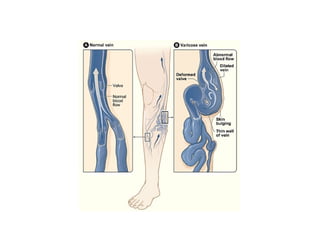
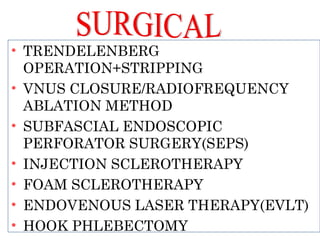






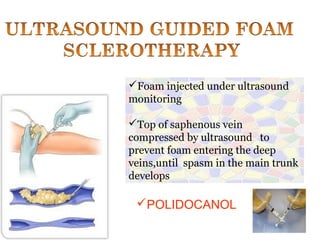
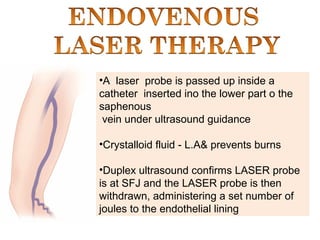
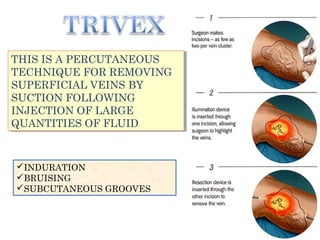




This document discusses varicose veins and their treatment options. It begins by describing the anatomy of varicose veins and their branches. It then discusses various surgical treatment options for varicose veins including stripping, endovenous laser therapy (EVLT), sclerotherapy, and hook phlebectomy. It provides details on the procedures, risks, post-operative care, and complications. In summary, it provides an overview of varicose vein anatomy and treatments through both invasive and non-invasive surgical procedures.



































































