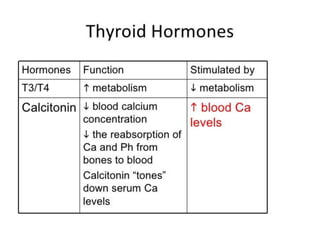
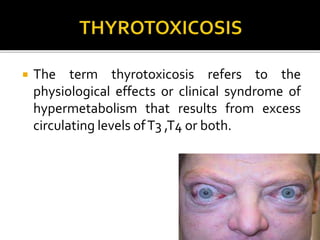
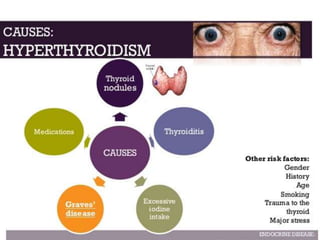
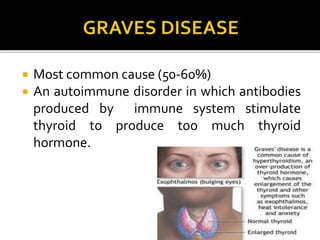
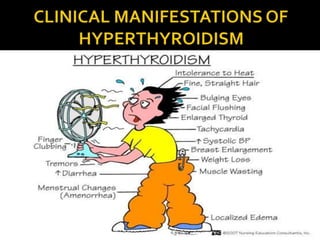
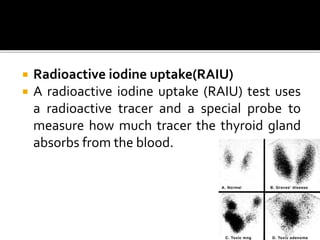
Hyperthyroidism is a condition where the thyroid gland produces excess thyroid hormones, causing a hypermetabolic state known as thyrotoxicosis. The most common cause is Graves' disease, an autoimmune disorder. Symptoms include weight loss, rapid heartbeat, sweating and irritability. Diagnosis involves blood tests to check thyroid hormone levels and treatment options include antithyroid medications, radioactive iodine therapy or surgery. Left untreated, hyperthyroidism can lead to complications affecting various body systems and organs.


















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




