Downloaded 118 times

















![Treatment – Medical – Beta-blockers
■ Pregnancy- absolute contraindication
■ Graves’ disease – goal is hypothyroidism after treatment
– Fixed dose or calculation (weight [g] x 150 µCi/g x 1/24 hour uptake %)
■ Toxic MNG andToxic Adenoma – can be euthyroid following treatment
■ May repeat in 6 months if initial dose not effective](https://image.slidesharecdn.com/hyperthyroidisminchildren-200824025958/75/Hyperthyroidism-in-children-43-2048.jpg)


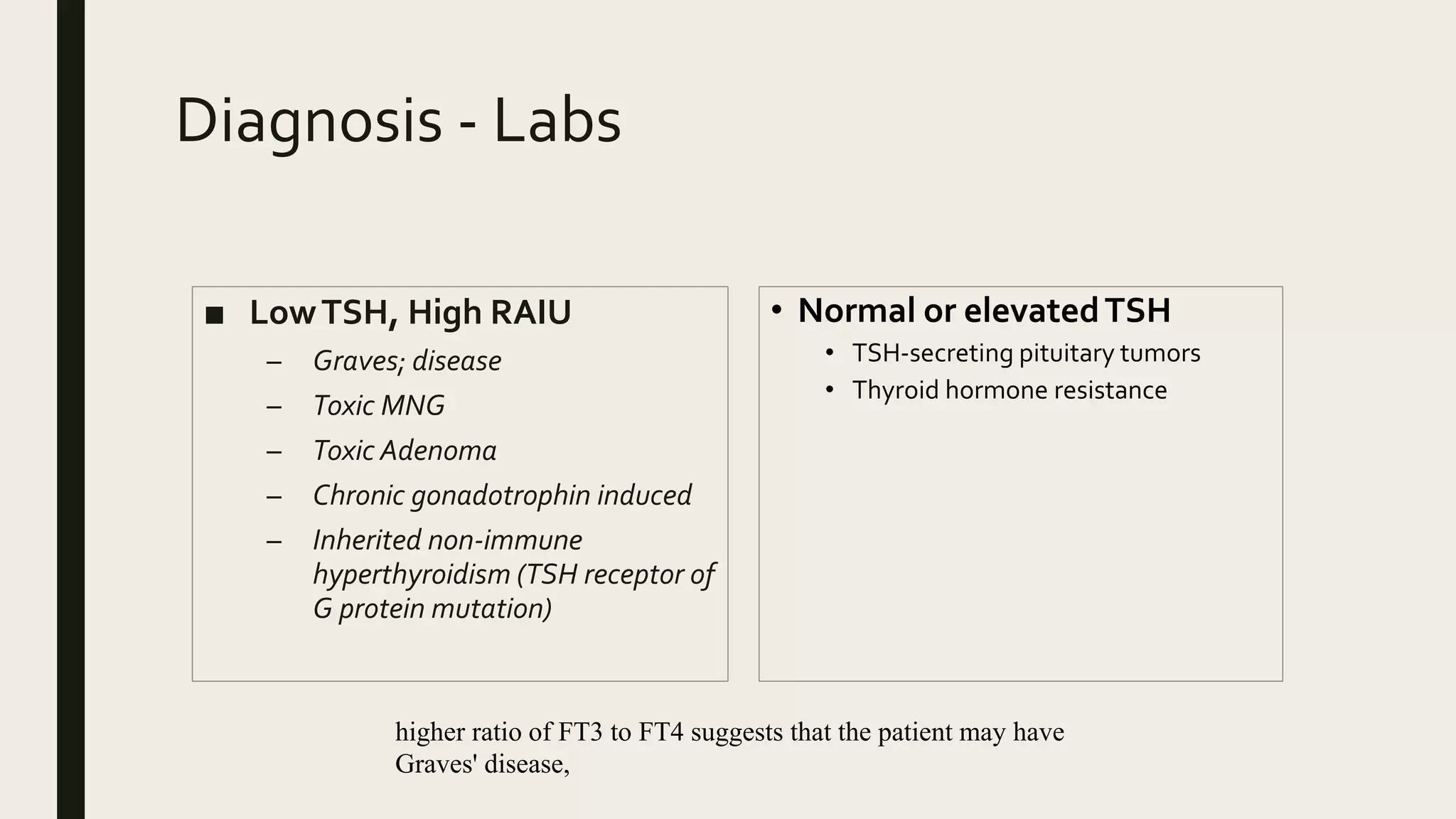
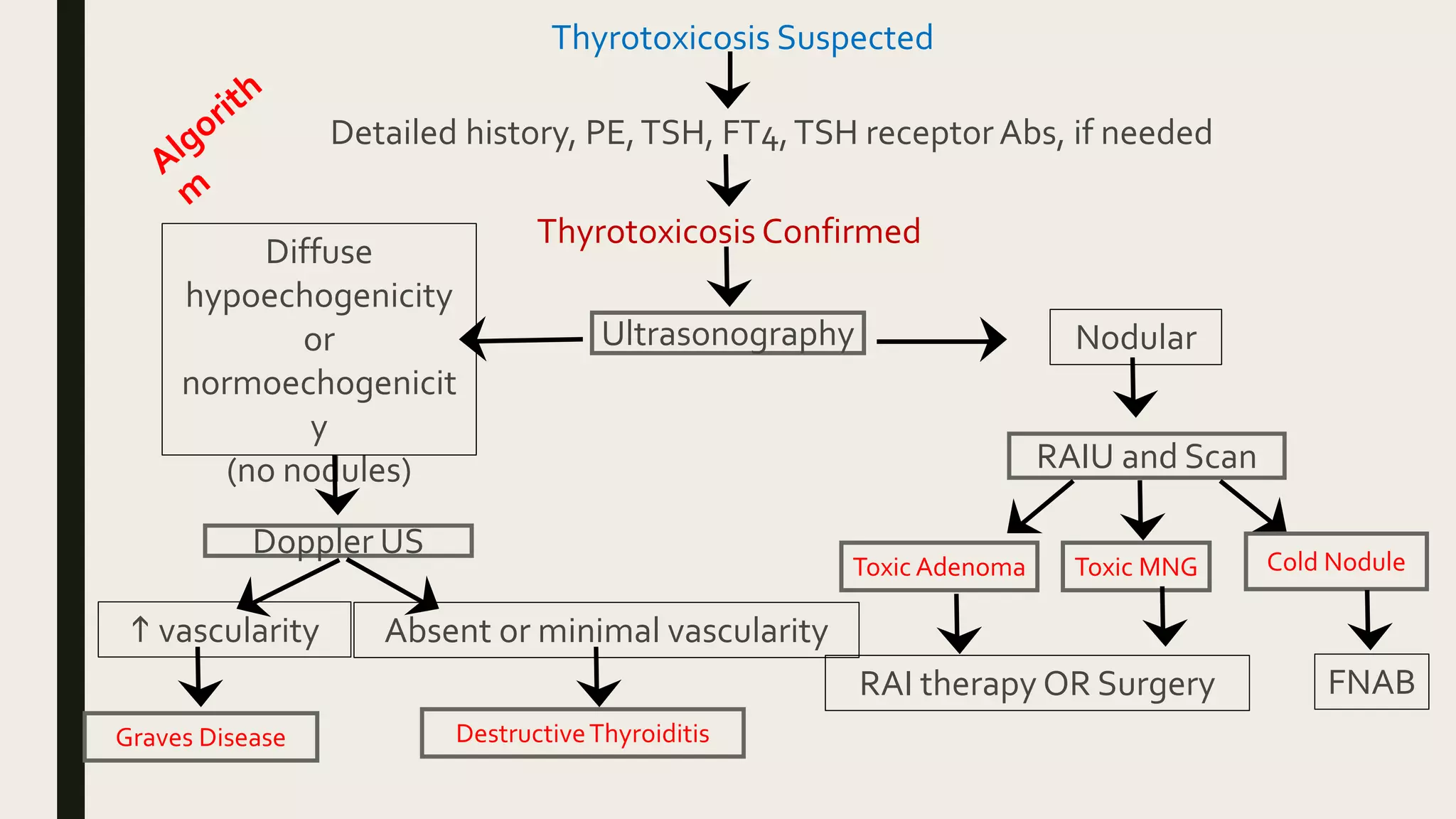
This document provides information on hyperthyroidism in children, including definitions, epidemiology, causes, clinical features, diagnosis, and management. The most common causes of hyperthyroidism in children are Graves' disease, toxic multinodular goiter, and subacute thyroiditis. Symptoms can include excessive sweating, heat intolerance, rapid heart rate, tremors, and weight loss. Diagnosis involves testing thyroid hormone levels, TSH, and thyroid antibodies. Treatment options include beta-blockers for symptom relief, antithyroid medications, radioactive iodine, and surgery. The goals of treatment are to normalize thyroid hormone levels and resolve symptoms of hyperthyroidism.























































































