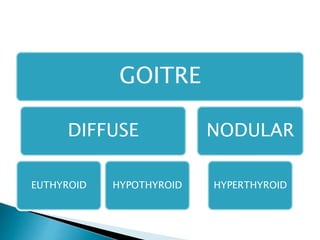
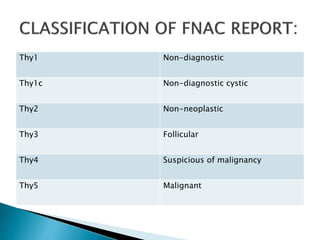
This document discusses different types of goiters including diffuse, nodular, hyperthyroid, and neoplastic goiters. It describes the causes of goiters such as iodine deficiency, dyshormonogenesis, and goitrogens. Evaluation of goiters involves assessing thyroid function tests, ultrasound characteristics, and fine needle aspiration cytology. Surgical treatment options for goiters include hemithyroidectomy, total/completion thyroidectomy, and management of substernal goiters.

















































































![Thyroid pathophysiology scintigraphy[1]](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidpathophysiologyscintigraphy1-161007125709-thumbnail.jpg?width=640&height=640&fit=bounds)