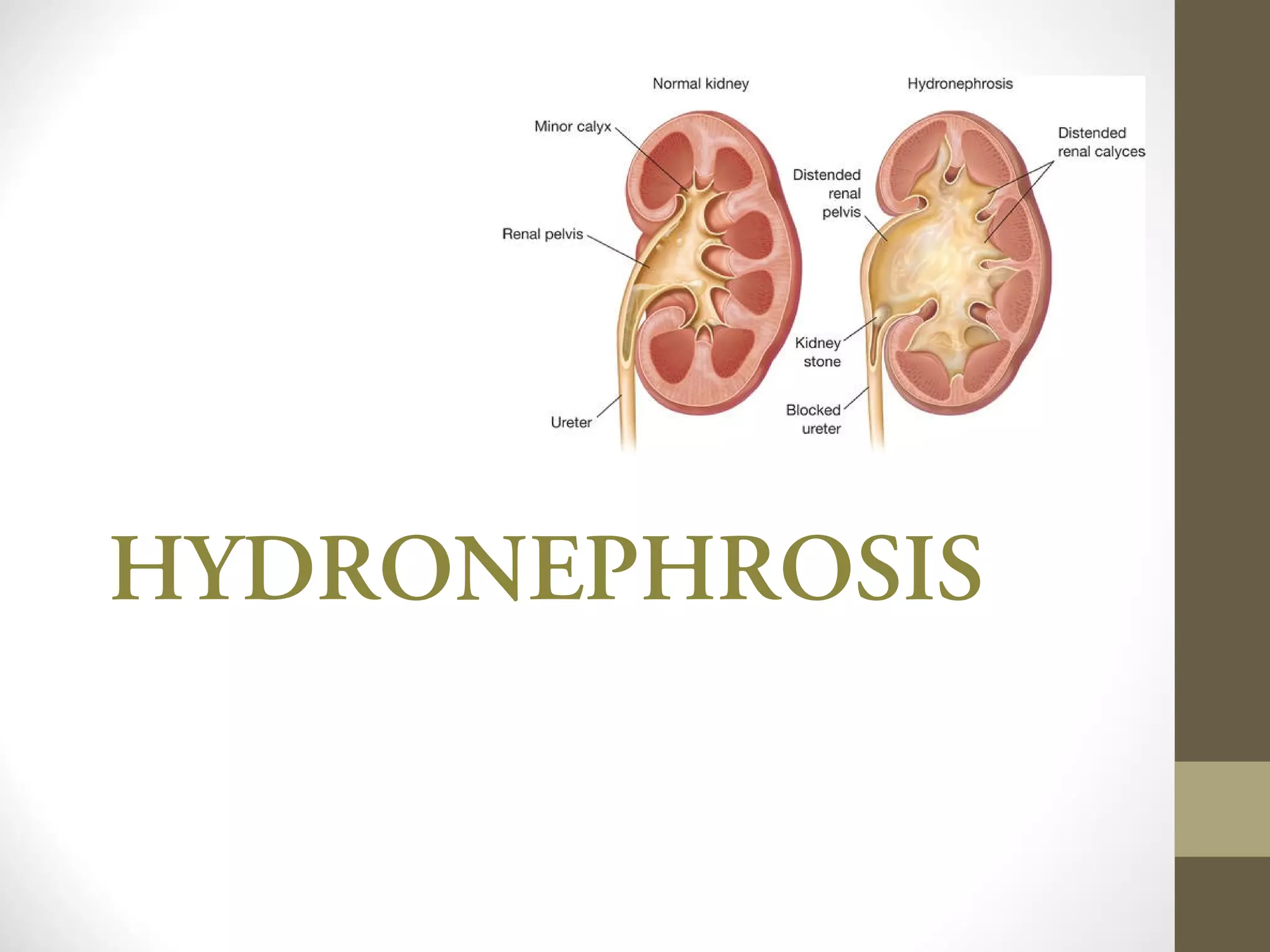
Hydronephrosis is the dilation of the renal pelvis and calyces caused by obstruction of urine flow from the kidney. It can be caused by issues in the ureter, bladder, or urethra that limit urine outflow. Unilateral hydronephrosis may cause dull flank pain while bilateral obstruction can lead to decreased urine output. Left untreated, hydronephrosis can damage kidney tissue and impair renal function. Diagnosis is made through imaging tests like intravenous pyelogram. Treatment focuses on resolving the underlying cause of obstruction.