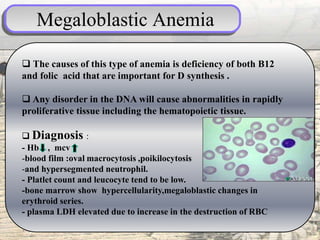
Pallor is a pale skin color caused by reduced oxyhemoglobin levels. It can be caused by anemia, leukemia, heart disease, shock, endocrine disorders, and more. Anemia itself is a reduction in red blood cells, hemoglobin, or red blood cell volume. The most common type is iron deficiency anemia from inadequate iron intake or absorption. Other types include megaloblastic anemia from B12 or folate deficiency, hemolytic anemia from red blood cell membrane issues or immune/non-immune causes, aplastic anemia from bone marrow failure, and anemia of chronic disease seen in infections, inflammation, or cancers.