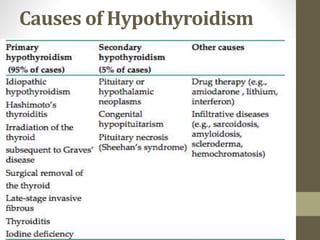
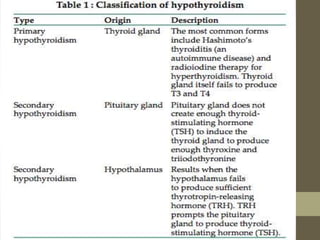
![Epidemiology
• The National Health and Nutrition Examination Survey
(NHANES 1999-2002) of 4392 individuals3.7%
hypothyroid. (defined as TSH levels exceeding 4.5
mIU/L)[22]
• World Health Organization (WHO) data from 130
countries taken from January 1994 through December
2006 found inadequate iodine nutrition in 30.6% of the
population.
• WHOurinary iodine concentrations100 to 199 μg/L
in the general population.
• 150-249 μg/L in pregnant women.](https://image.slidesharecdn.com/thyroid-140605130618-phpapp02/85/HYPOTHYROID-10-320.jpg)
![• Age-related demographics:The frequency increases with
age.
• Most prevalent in elderly populations-The Framingham
study found hypothyroidism (TSH > 10 mIU/L) in 5.9% of
women and 2.4% of men older than 60 years.[24]
• Sex-related demographics:2 to 8 times higher in females.
• Race-related demographics:NHANES 1999-2002 whites
(5.1%) and Mexican Americans than in African Americans
(1.7%).](https://image.slidesharecdn.com/thyroid-140605130618-phpapp02/85/HYPOTHYROID-11-320.jpg)
![Postpartum thyroiditis
• Up to 10% of postpartum develop lymphocytic thyroiditis in the
2-12 months after delivery.
• Transient (2-4 months).
• Increased risk of permanent hypothyroidism or recurrence of
postpartum thyroiditis with future pregnancies.
• In a 12-year longitudinal study, Stuckey et al found that
hypothyroidism developed in 27 of 71 women (38%) who had a past
history of postpartum thyroid dysfunction (PPTD). In comparison,
only 14 of 338 women (4%) who had not had PPTD developed
hypothyroidism.[5]](https://image.slidesharecdn.com/thyroid-140605130618-phpapp02/85/HYPOTHYROID-16-320.jpg)
![Drug-induced& iatrogenichypothyroidism
• The following medications reportedly have the potential to cause
hypothyroidism:
• Iodine excess (including iodine-containing contrast media and
amiodarone),
• lithium,
• antithyroid drugs,
• p-aminosalicylic acid,
• interferon-
• tyrosine kinase inhibitors – Sunitinib, imatinib[6]
• Bexarotene[7]](https://image.slidesharecdn.com/thyroid-140605130618-phpapp02/85/HYPOTHYROID-18-320.jpg)
![Genetics
• Genome-wide association studies FOXE1 gene hypothyroidism.
• 10% of patients with congenital hypothyroidism have an error in
thyroid hormone synthesis.[9]
• Mutations in the TPO gene appear to be the most common error of
hormone synthesis, causing failure to produce adequate amounts of
TPO.[10]
• Mutations in the TSHR and PAX8 genes congenital hypothyroidism
without goiter.[11, 12]](https://image.slidesharecdn.com/thyroid-140605130618-phpapp02/85/HYPOTHYROID-20-320.jpg)
![• Pendred syndrome mutation in the SLC26A4 gene defect in
the organification of iodine
congenital sensorineural hearing loss,
enlarged thyroid gland.
autosomal recessive manner.[13]
• Autoimmune polyendocrinopathy
typeIAIRE genecharacterized by the presence of Addison
disease, hypoparathyroidism, and mucocutaneous candidiasis.
• Autoimmune polyendocrinopathy type 2 (Schmidt syndrome) is
associated with adrenal insufficiency and hypothyroidism](https://image.slidesharecdn.com/thyroid-140605130618-phpapp02/85/HYPOTHYROID-21-320.jpg)
![Iodine deficiency or excess
• Most common cause of hypothyroidism. Excess iodine can transiently
inhibit iodide organification and thyroid hormone synthesis (the
Wolff-Chiakoff effect).
• Healthy individualsphysiologic escape from this effect. In patients
with iodine overloadsodium-iodide symporter shuts downallows
intracellular iodine levels to drop and hormone secretion to resume.
• The Wolff-Chiakoff effect is short-livedsodium-iodide symporter is
capable of rapidly downregulation.
• exposure to excess iodineprofound and sustained hypothyroidism
in individuals with abnormal thyroid glands.[15]](https://image.slidesharecdn.com/thyroid-140605130618-phpapp02/85/HYPOTHYROID-22-320.jpg)
![Central hypothyroidism[16, 17]
• Central hypothyroidismhypothalamic-pituitary axis is
damaged. The following potential causes should be
considered :
Pituitary adenoma-exerting pressure on normal
pituitary cells
Tumors impinging on hypothalamus
Lymphocytic hypophysitis- cause death of cells.
Sheehan syndrome
History of brain or pituitary irradiation](https://image.slidesharecdn.com/thyroid-140605130618-phpapp02/85/HYPOTHYROID-24-320.jpg)
![• Drugs (eg, dopamine, prednisone, or opioids)-decreased TSH
secretion.
• Congenital non goiterous hypothyroidism type 4Mutation in
theTSHB geneautosomal recessive pattern
• TRH resistanceTRHR geneautosomal recessive manner.
hypothyroidism and, unsurprisingly, have insensitivity to
thyrotropin secretion.[19]
• TRH deficiencymutation in the TRH geneautosomal recessive
manner.[20]](https://image.slidesharecdn.com/thyroid-140605130618-phpapp02/85/HYPOTHYROID-25-320.jpg)
![5-Stuckey BG, Kent GN, Ward LC, Brown SJ, Walsh JP. Postpartum thyroid
dysfunction and the long-term risk of hypothyroidism: results from a 12-year
follow-up study of women with and without postpartum thyroid
dysfunction. Clin Endocrinol (Oxf). Sep 2010;73(3):389-95. [Medline].
6-Wolter P, Dumez H, Schöffski P. Sunitinib and hypothyroidism. N Engl J
Med. Apr 12 2007;356(15):1580; author reply 1580-1. [Medline].
Smit JW, Stokkel MP, Pereira AM, Romijn JA, Visser TJ. Bexarotene-induced
hypothyroidism: bexarotene stimulates the peripheral metabolism of thyroid
hormones. J Clin Endocrinol Metab. Jul 2007;92(7):2496-9. [Medline].
9-Vono-Toniolo J, Rivolta CM, Targovnik HM, Medeiros-Neto G, Kopp P.
Naturally occurring mutations in the thyroglobulin gene. Thyroid. Sep
2005;15(9):1021-33. [Medline].
10-Park SM, Chatterjee VK. Genetics of congenital hypothyroidism. J Med
Genet. May 2005;42(5):379-89.[Medline]. [Full Text].
11-Paschke R, Ludgate M. The thyrotropin receptor in thyroid diseases. N Engl J
Med. Dec 4 1997;337(23):1675-81. [Medline].](https://image.slidesharecdn.com/thyroid-140605130618-phpapp02/85/HYPOTHYROID-55-320.jpg)
![12-Macchia PE, Lapi P, Krude H, Pirro MT, Missero C, Chiovato L, et al.
PAX8 mutations associated with congenital hypothyroidism caused by
thyroid dysgenesis. Nat Genet. May 1998;19(1):83-6. [Medline].
13-Everett LA, Glaser B, Beck JC, Idol JR, Buchs A, Heyman M, et al.
Pendred syndrome is caused by mutations in a putative sulphate
transporter gene (PDS). Nat Genet. Dec 1997;17(4):411-22. [Medline].
15-Woeber KA. Iodine and thyroid disease. Med Clin North Am. Jan
1991;75(1):169-78. [Medline]
16-Yamada M, Mori M. Mechanisms related to the pathophysiology
and management of central hypothyroidism. Nat Clin Pract Endocrinol
Metab. Dec 2008;4(12):683-94. [Medline].
17-Nebesio TD, McKenna MP, Nabhan ZM, Eugster EA. Newborn
screening results in children with central hypothyroidism. J Pediatr. Jun
2010;156(6):990-3. [Medline].
19-Bonomi M, Busnelli M, Beck-Peccoz P, Costanzo D, Antonica F, Dolci
C, et al. A family with complete resistance to thyrotropin-releasing
hormone. N Engl J Med. Feb 12 2009;360(7):731-4. [Medline].
20-Katakami H, Kato Y, Inada M, Imura H. Hypothalamic
hypothyroidism due to isolated thyrotropin-releasing hormone (TRH)
deficiency. J Endocrinol Invest. Jun 1984;7(3):231-3. [Medline].](https://image.slidesharecdn.com/thyroid-140605130618-phpapp02/85/HYPOTHYROID-56-320.jpg)


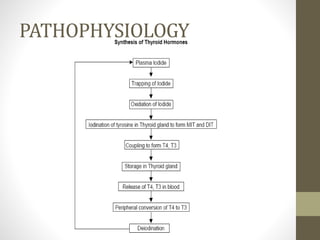
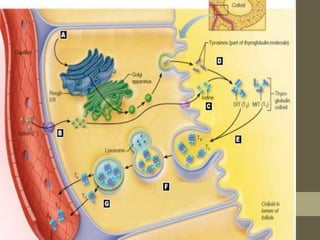
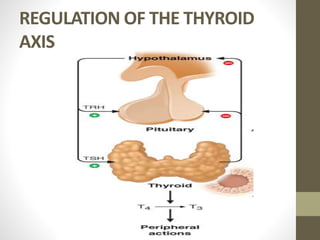
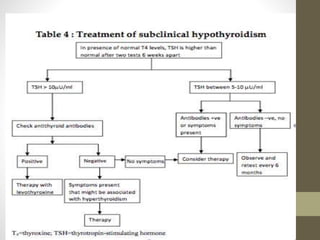
This document provides an overview of hypothyroidism, including: 1. It discusses the anatomy and function of the thyroid gland and describes primary causes of hypothyroidism like chronic lymphocytic thyroiditis and iodine deficiency. 2. Laboratory tests for assessing hypothyroidism are outlined, with TSH identified as the most specific indicator. Conditions that can alter TSH and thyroid hormone levels are also noted. 3. The clinical presentation of hypothyroidism is reviewed along with treatment considerations like increased thyroid hormone needs during pregnancy. Biochemical markers and expected signs of clinical improvement with treatment are summarized.

























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





