Downloaded 331 times






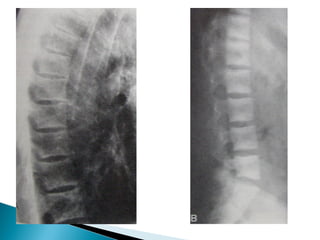

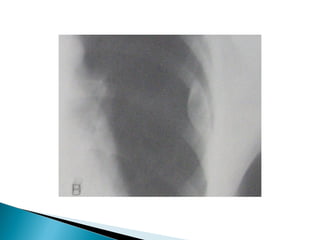

The document discusses primary hyperparathyroidism, which is caused by adenomas, hyperplasia, or carcinoma of the parathyroid glands. It causes increased calcium absorption and bone resorption while promoting calcium and phosphate excretion in the kidneys. Symptoms include kidney stones, bone loss, fatigue, and abdominal pain. Diagnosis involves blood tests showing elevated calcium and PTH levels. Treatment is parathyroidectomy for severe cases.






































































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)




