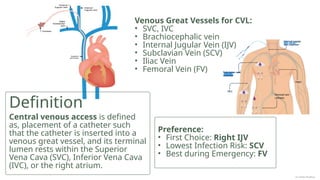
Central venous access involves placing a catheter into a venous great vessel.
The terminal end of the catheter rests in the SVC, IVC, or right atrium.
Common insertion sites are the Internal Jugular Vein (IJV), Subclavian Vein (SCV), or Femoral Vein (FV).
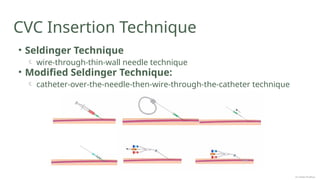
Insertion often utilizes the Modified Seldinger Technique. Real-time USG guidance is recommended for the procedure.
Post-procedure Chest X-ray (CXR) confirms tip position and checks for complications like pneumothorax.
Infection prevention is the utmost priority in care


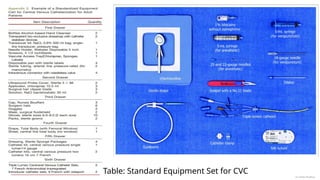
![CVC Procedural Steps
Patient Positioning: Trendelenburg (IJ & SC
access); Supine (Femoral access)
Aseptic Preparation
USG Identification [IJV: Compressible, non
pulsatile vessel, lateral to carotid]
Local Anesthesia [field flooded with LA, distorts
anatomy]
Venous Puncture under USG guidance [must
visualize the needle entering the vein; aspirate
dark, non-pulsatile blood to confirm]
Dr Jebish Pradhan](https://image.slidesharecdn.com/cvcinsertionjebish-251214155450-e4c97983/85/Central-Venous-Line-Insertion-Technique-Complications-8-320.jpg)
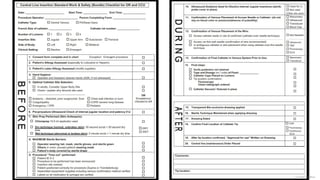
![CVC Procedural Steps
Guidewire Insertion [over a stable needle,
advanced slowly; if resistance, stop & recheck
needle position; confirm wire in the vein with USG]
Remove Needle [Wire kept straight and stable by
holding firmly with other hand]
Skin Nick beside wire [facilitate entry point for
dilator and CVC]
Dilatation [advance dilator over wire with twisting
motion gently]
Catheter Insertion [over the wire, to measured
depth; ~15cm Rt IJV to SVC / push until hub
Dr Jebish Pradhan](https://image.slidesharecdn.com/cvcinsertionjebish-251214155450-e4c97983/85/Central-Venous-Line-Insertion-Technique-Complications-9-320.jpg)
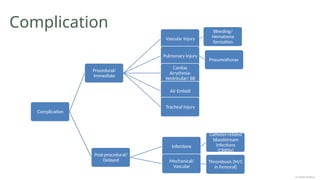
![CVC Procedural Steps
Aspiration and Flushing of each lumen
Secure [2 sutures to secure catheter to skin]
Dressing [Sterile Transparent Dressing]
CXR [confirm tip position & r/o Pneumothorax]
Clear Documentation
Dr Jebish Pradhan](https://image.slidesharecdn.com/cvcinsertionjebish-251214155450-e4c97983/85/Central-Venous-Line-Insertion-Technique-Complications-10-320.jpg)
![• Practice Guidelines for Central Venous Access 2020: An Updated Report
by the American Society of Anesthesiologists Task Force on Central
Venous Access*. Anesthesiology 132(1):p 8-43, January 2020. | DOI:
10.1097/ALN.0000000000002864
• Kolikof J, Peterson K, Williams C, et al. Central Venous Catheter Insertion.
[Updated 2025 Feb 4]. In: StatPearls [Internet]. Treasure Island (FL):
StatPearls Publishing; 2025 Jan-. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK557798/
• Australian and New Zealand Intensive Care Society. Central Line
Insertion and Maintenance Guideline. Melbourne: ANZICS; 2012.
Available from:
https://www.anzics.org/wp-content/uploads/2018/08/ANZICS_Insertion
maintenance_guideline2012_04.pdf.
References
Dr Jebish Pradhan](https://image.slidesharecdn.com/cvcinsertionjebish-251214155450-e4c97983/85/Central-Venous-Line-Insertion-Technique-Complications-14-320.jpg)








































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







