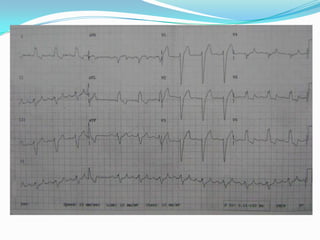
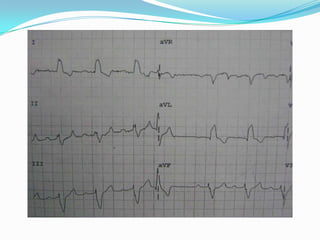
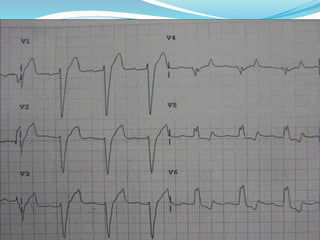
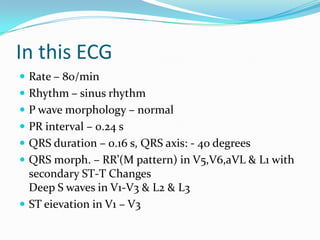
A 73-year-old male presented with dizziness for 1 year and chest pain for 2 days. His ECG showed left bundle branch block (LBBB) and first-degree atrioventricular block, consistent with possible trifascicular block. Trifascicular block must be confirmed with bundle of His electrogram. The patient has abnormal conduction through one or more divisions of the intraventricular conduction system distal to the bundle of His, presenting as LBBB and first-degree AV block. This suggests involvement of the left and right bundles as well as the AV node, consistent with trifascicular block.
























































![Ecg [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/ecgautosaved-200407040542-thumbnail.jpg?width=640&height=640&fit=bounds)












































