Downloaded 6,042 times






























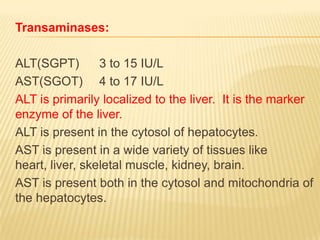








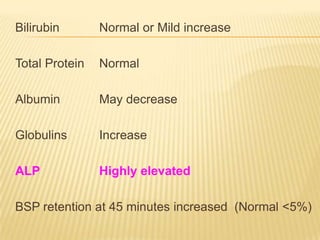


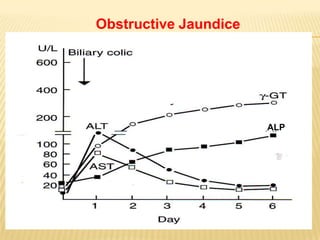




The document discusses liver function tests (LFTs) and their use in evaluating liver diseases. It provides details on 3 key LFTs: 1. Bilirubin tests which are used to diagnose prehepatic (hemolytic), hepatic, and obstructive jaundice. Elevated conjugated bilirubin indicates obstructive jaundice while elevated unconjugated bilirubin indicates hepatic or hemolytic jaundice. 2. Liver enzymes like ALT, AST, ALP, and GGT which provide information on liver health and injury. Elevated ALT and AST indicate liver parenchymal damage while elevated ALP and GGT can indicate obstructive jaundice. 3























































































