Downloaded 676 times
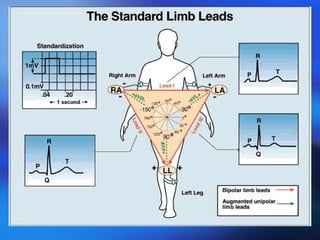
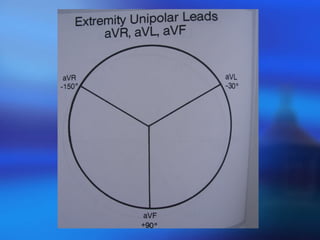
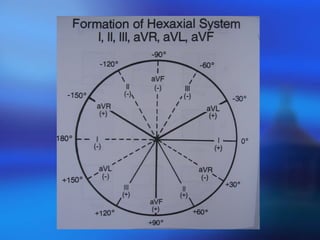
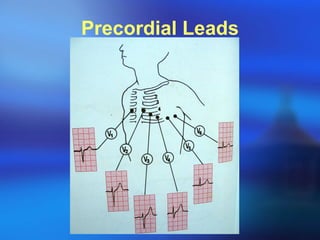
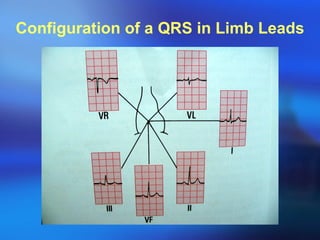
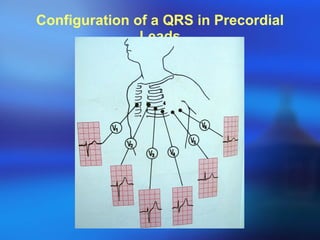
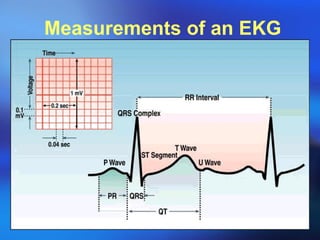
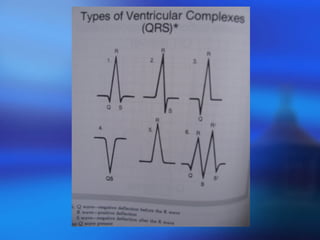
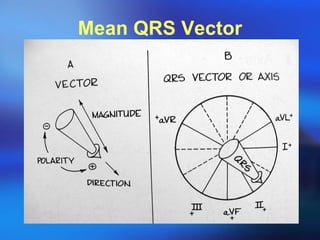

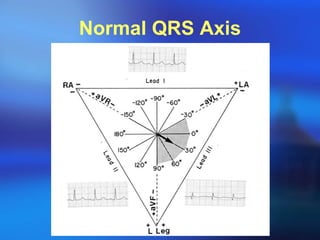
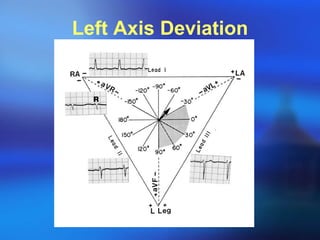
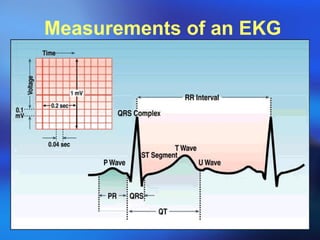
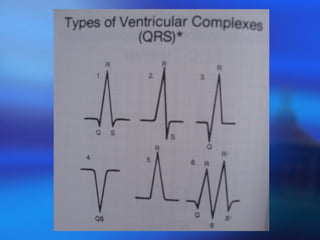
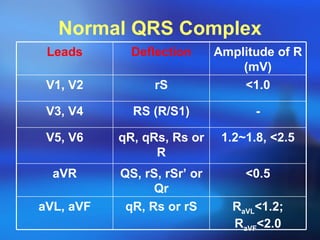
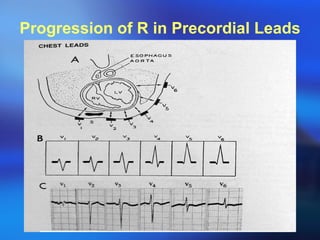
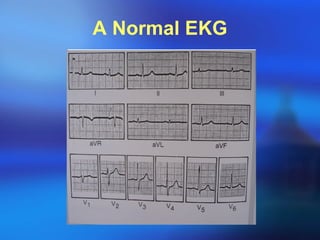
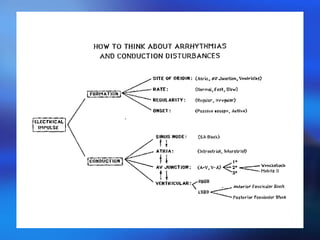
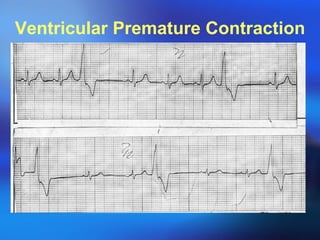
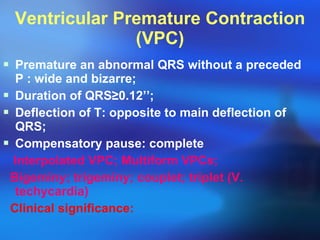
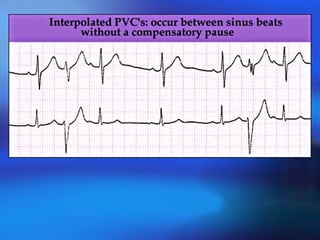
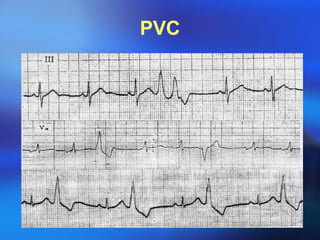
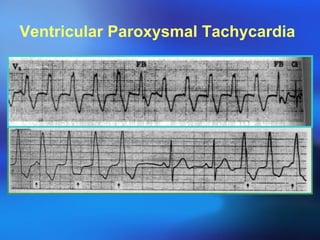
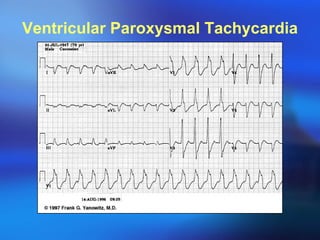
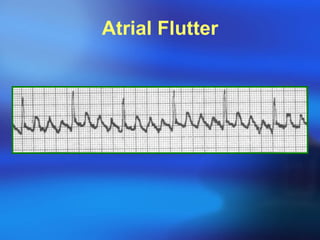
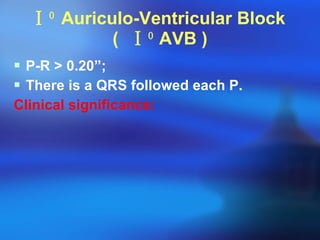


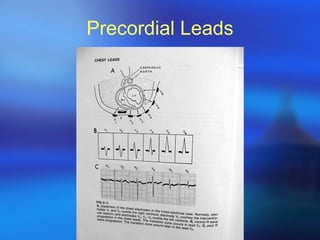
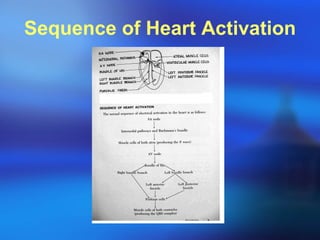

The document provides an overview of electrocardiography (ECG/EKG) including its uses in diagnosis, components of an ECG reading, normal values, abnormalities, and interpretations. Key aspects of ECG such as P waves, QRS complex, ST segment, T wave, and measurements including axes are defined. Common conditions involving the heart's rhythm and structure that can be identified on ECG are also summarized.




































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















