Downloaded 54 times
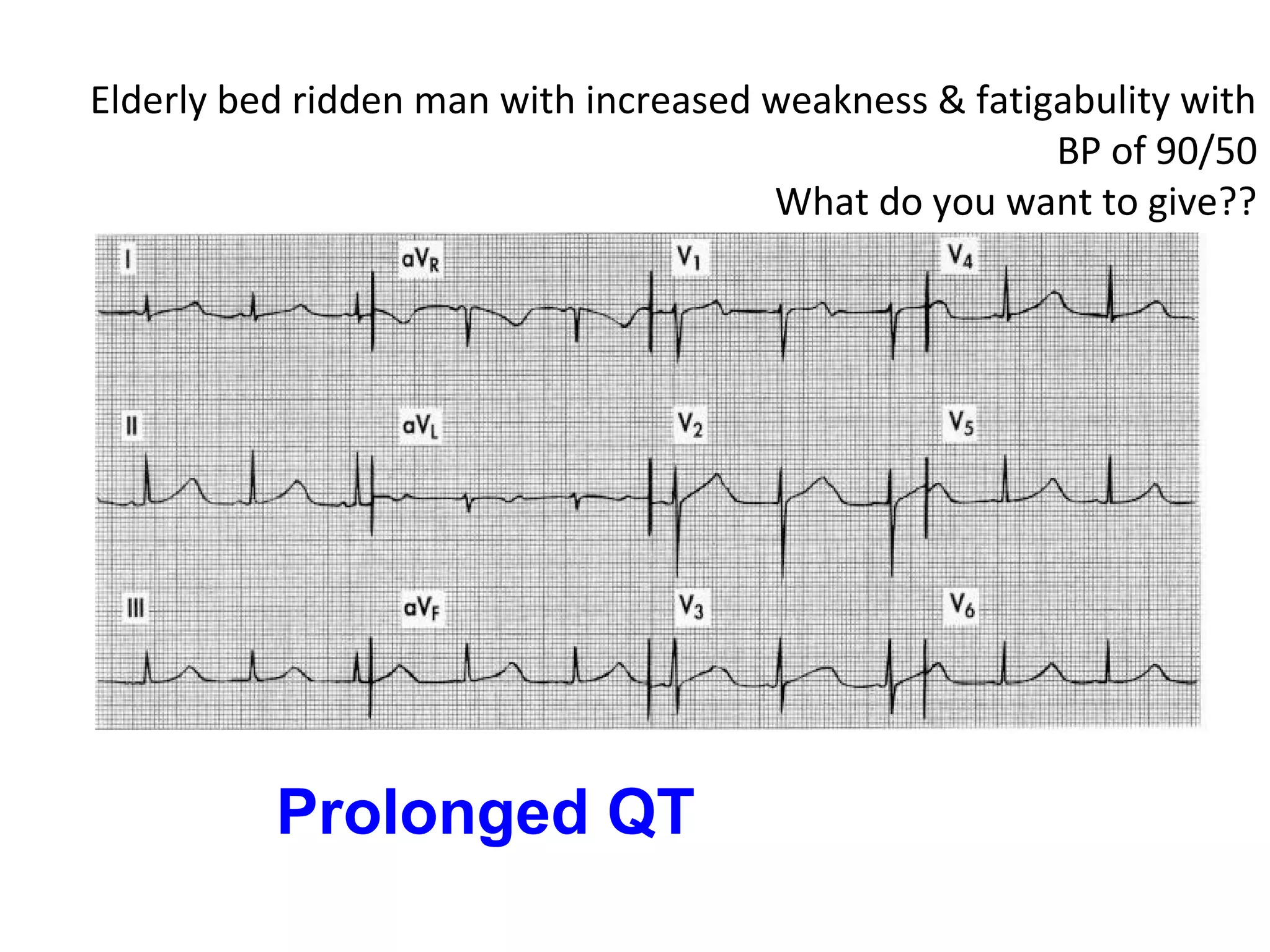
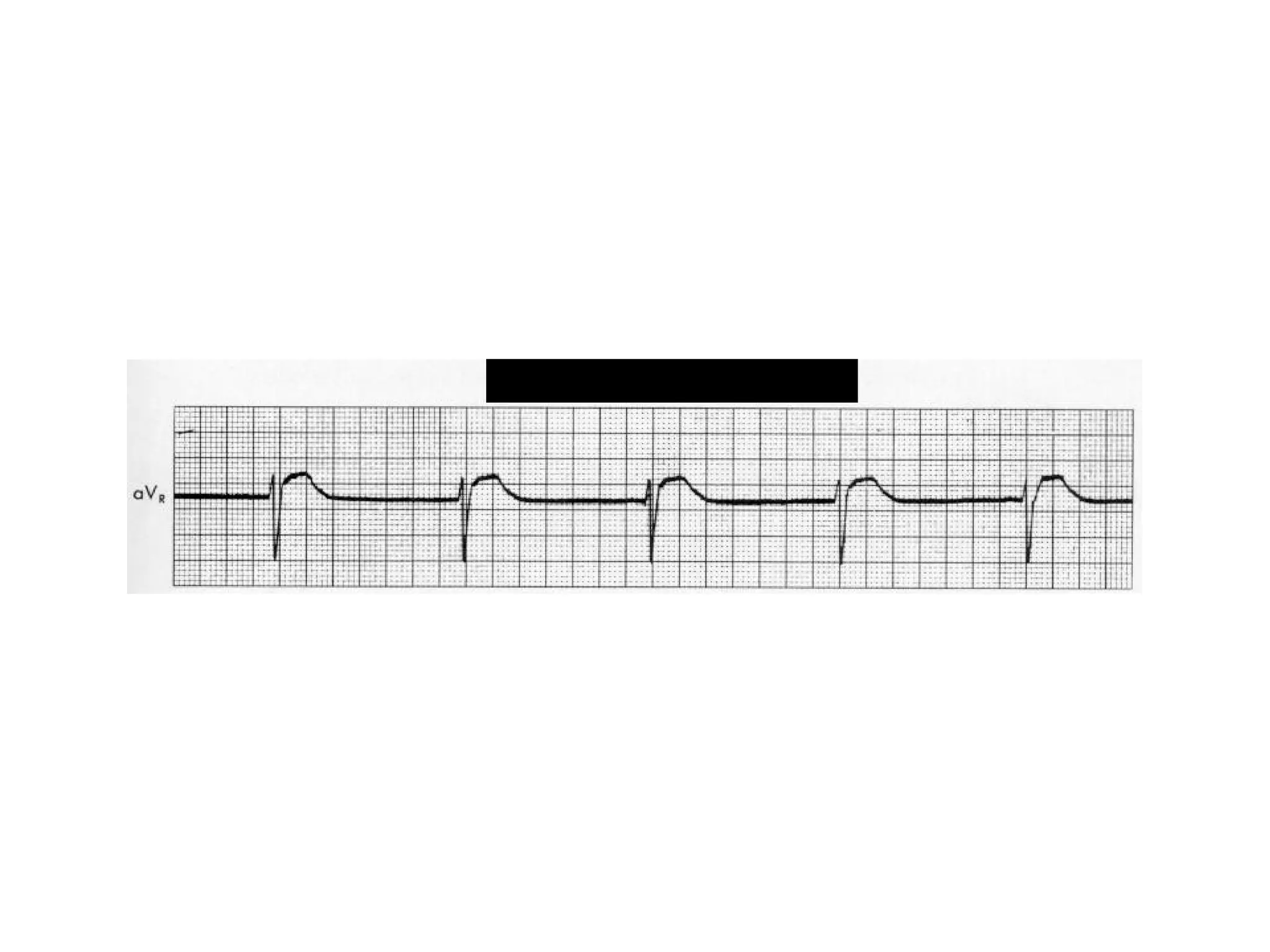
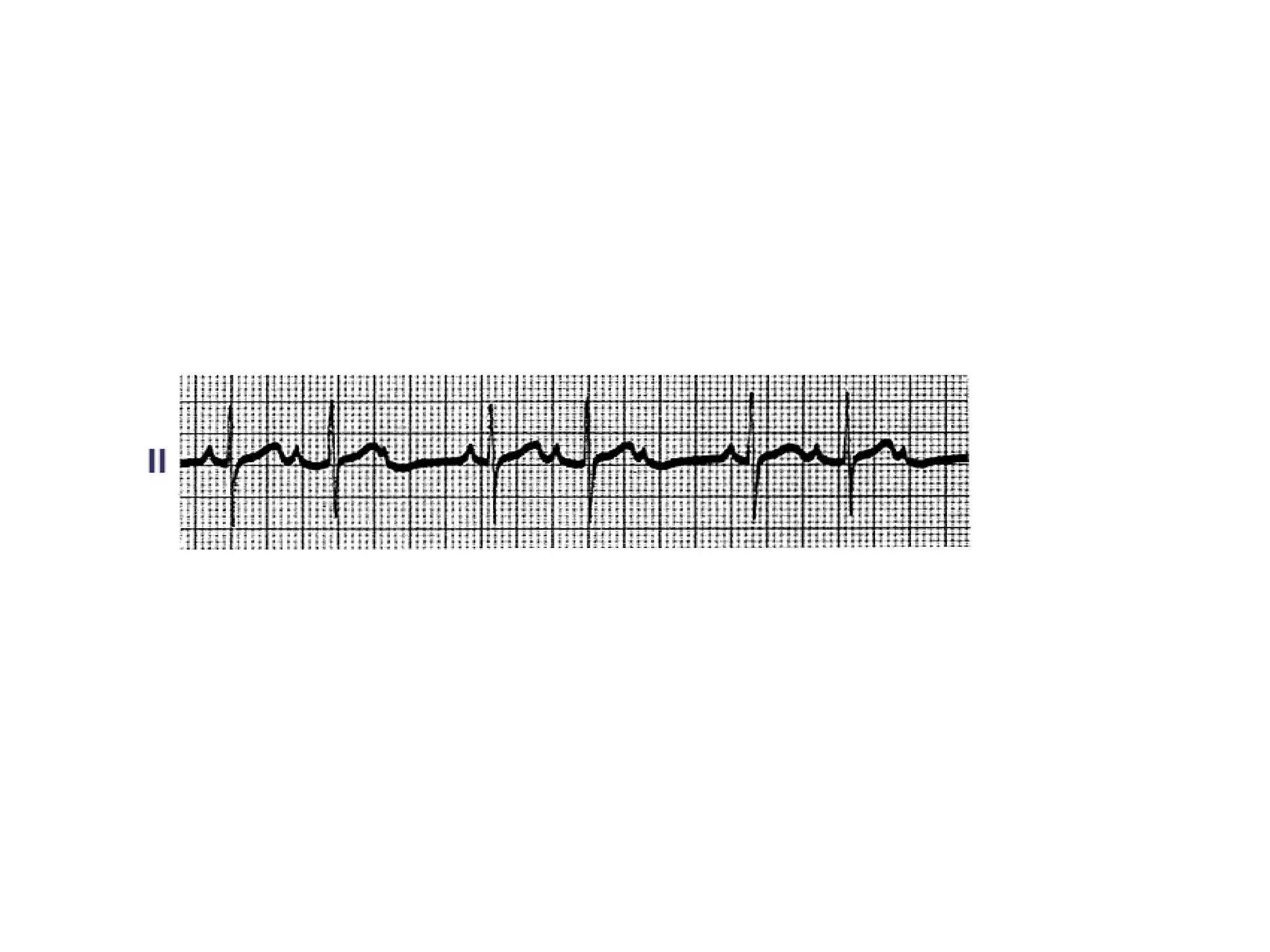
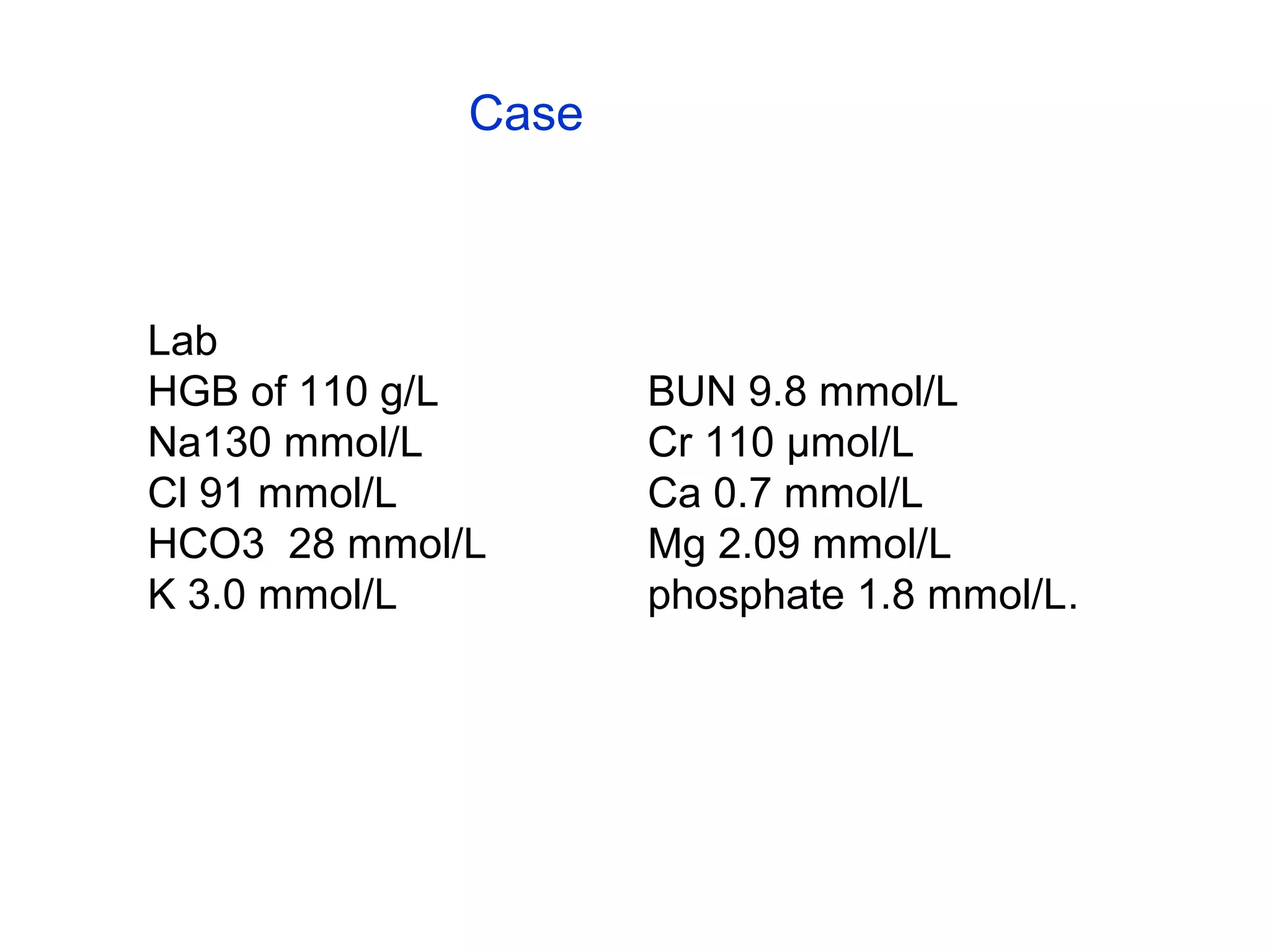
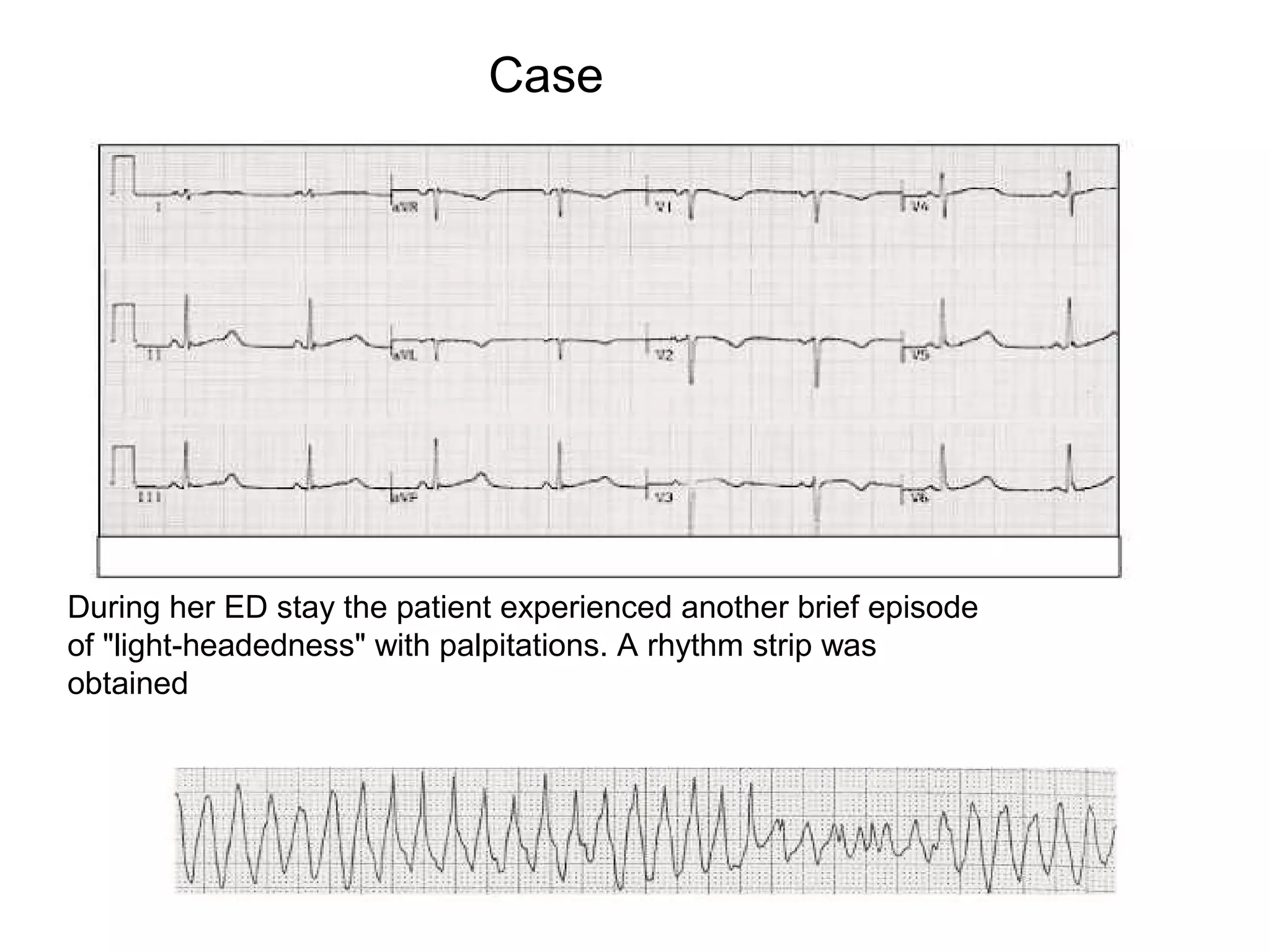

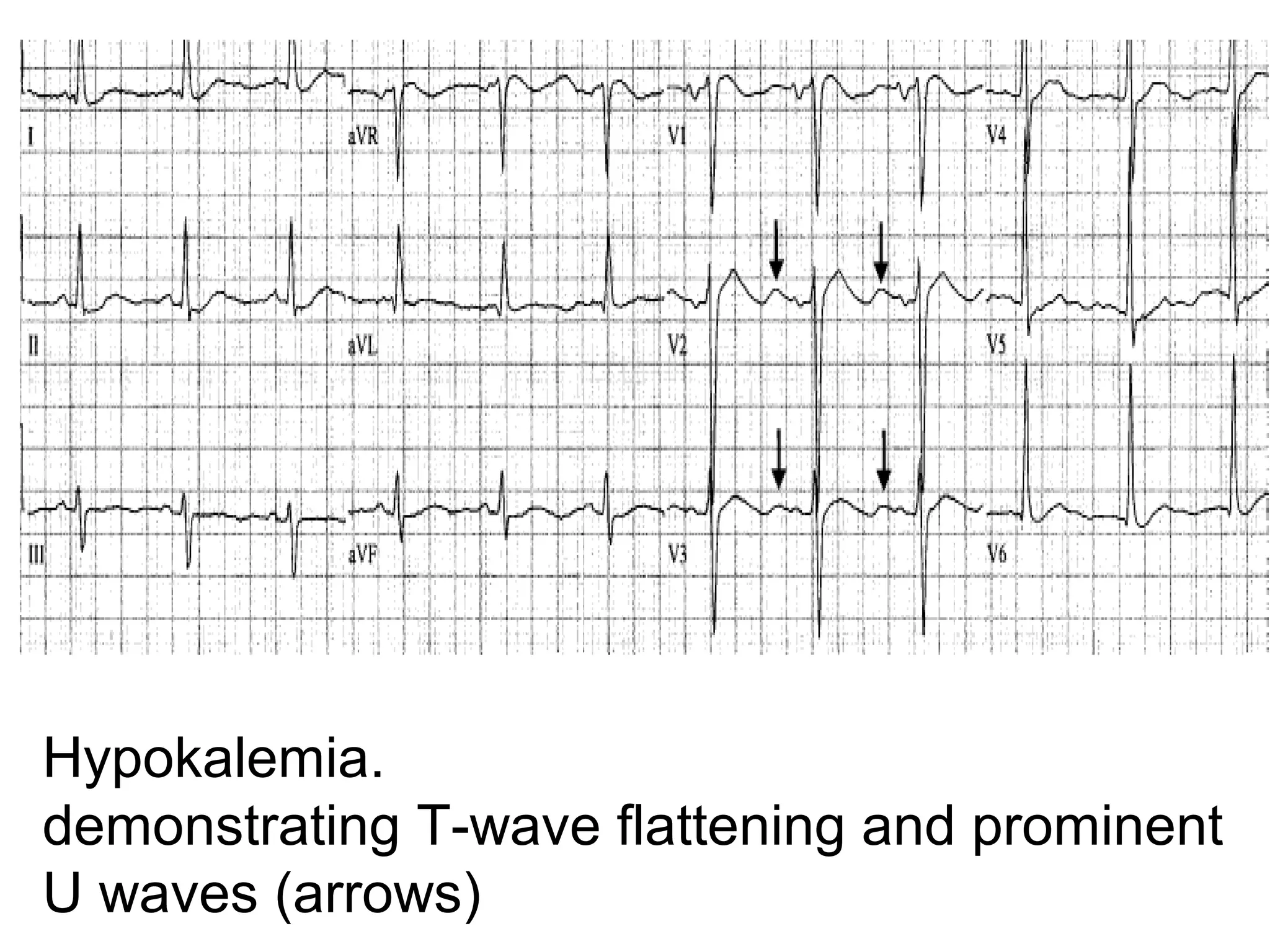

A 23-year-old female presented with episodes of feeling lightheaded and weak. She had a history of anorexia nervosa and had lost significant weight recently. Laboratory tests revealed low calcium, potassium, and other electrolyte abnormalities. During her emergency department stay, she experienced another episode where a rhythm strip was obtained. The rhythm strip showed a prolonged QT interval, likely the cause of her symptoms due to electrolyte abnormalities from her eating disorder.

































































![Ecg [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/ecgautosaved-200407040542-thumbnail.jpg?width=640&height=640&fit=bounds)









































