Downloaded 4,256 times




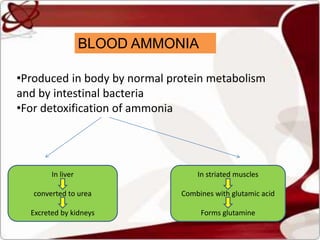
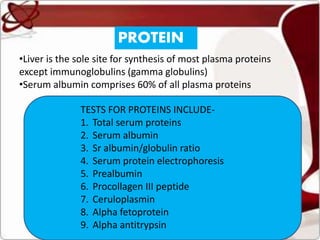
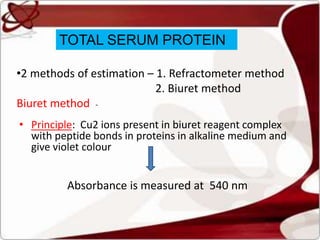

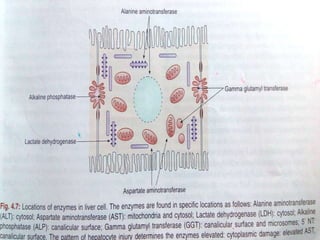

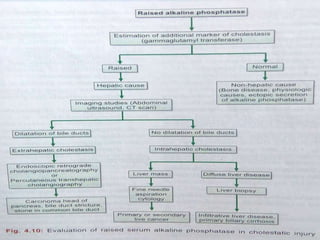


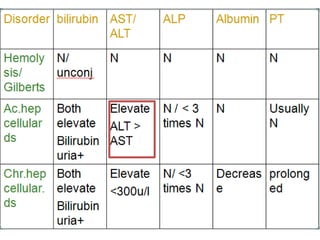
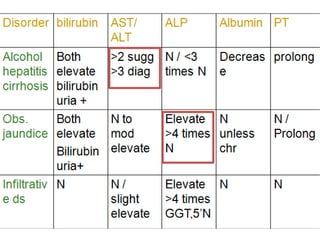


Liver function tests can detect, distinguish, and monitor various types of liver disease. Tests are grouped based on the liver's excretory, metabolic, detoxification, storage and synthetic functions. Enzyme tests like ALT and AST indicate hepatocyte damage, while elevated ALP and GGT suggest cholestasis. Protein tests such as albumin, PT and AFP evaluate synthetic function. Bilirubin, bile salts and dye excretion tests examine excretory function. Together these tests provide insight into liver health and disease categories.
















































































