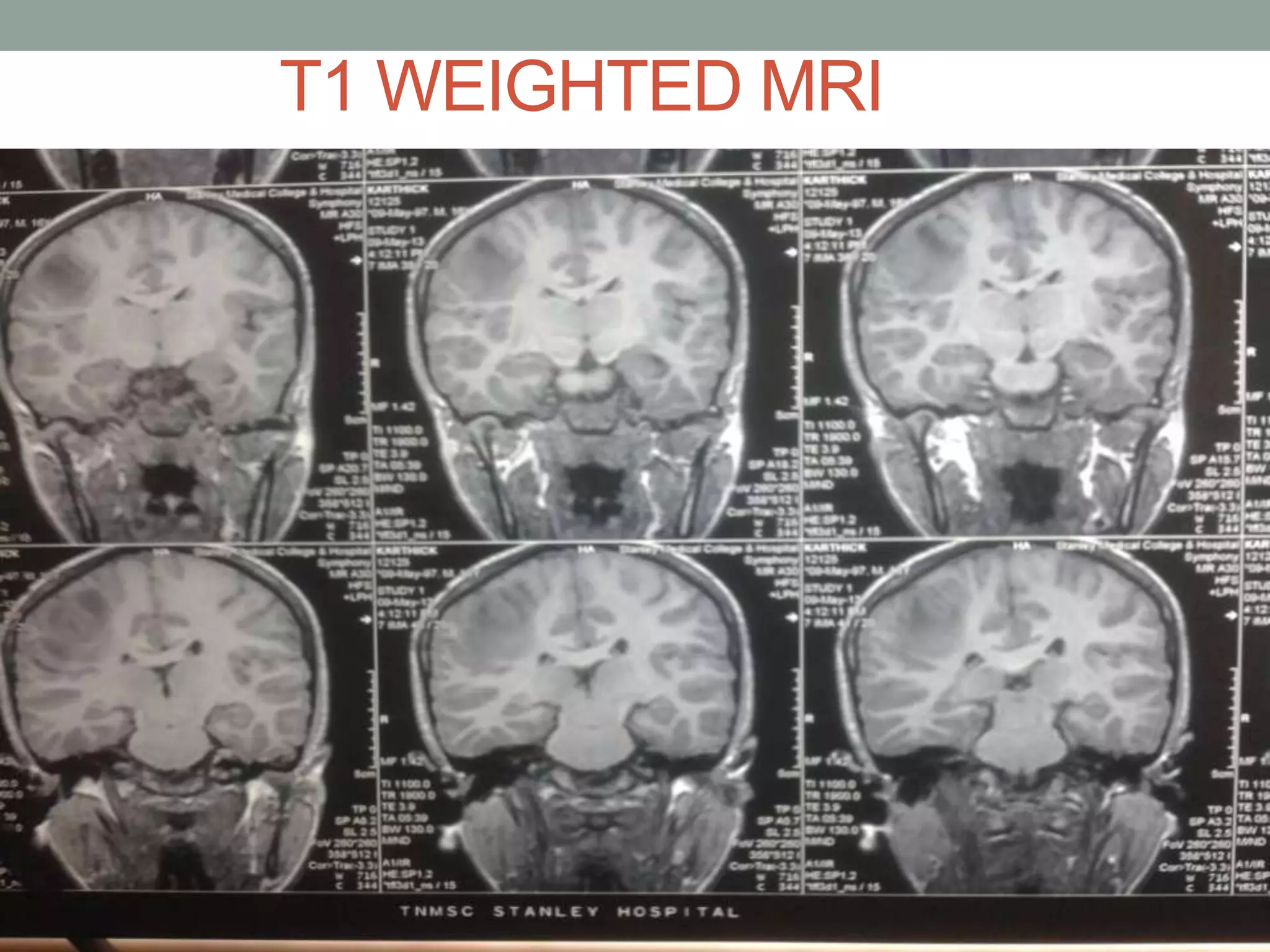
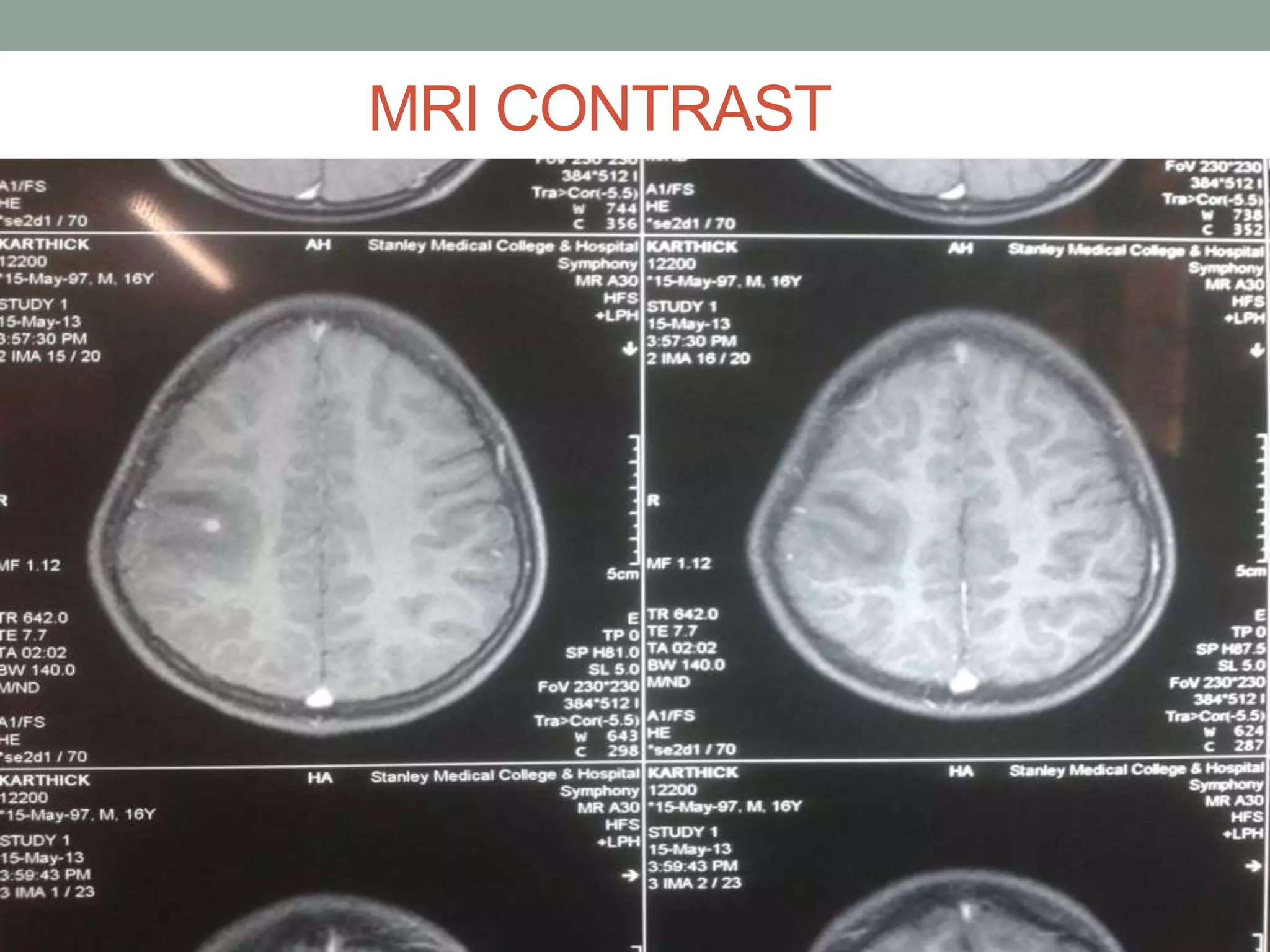
A 16-year-old boy was admitted with abnormal movements of his left thumb and left eyelid for over 1 hour. MRI scans showed lesions in his brain consistent with neurocysticercosis. Neurocysticercosis is caused by the pork tapeworm Taenia solium and has four pathogenic stages seen on imaging. The patient's symptoms, travel history, imaging findings, and positive blood tests confirmed a diagnosis of neurocysticercosis. He was treated with anti-seizure medications, anti-parasitic drugs, and steroids to reduce inflammation from degenerating parasites.