Downloaded 45 times
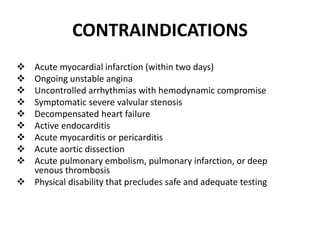



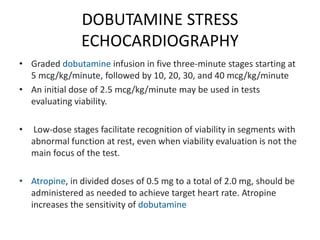

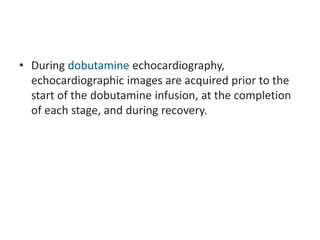

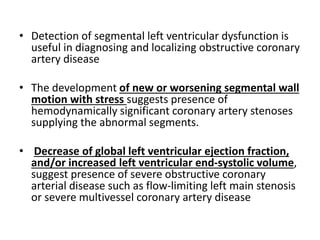
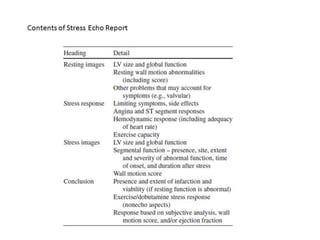

Stress echocardiography enables evaluation of cardiac function at rest and during exercise or pharmacologic stress. It can detect wall motion abnormalities indicative of ischemia and assess valvular function, left ventricular outflow tract gradients, and pulmonary pressures. Exercise or pharmacologic agents like dobutamine are used to induce stress. Indications include evaluating known or suspected coronary artery disease, viability, and valvular diseases. The test is contraindicated in acute coronary syndromes or hemodynamically significant valvular stenosis. Imaging is performed at rest and peak stress to detect new or worsening wall motion abnormalities. Doppler can also evaluate hemodynamic changes with stress.





































![Stresstesting housestaffdidactic_10092014[1]](https://cdn.slidesharecdn.com/ss_thumbnails/stress20testinghousestaff20didactic100920141-141013101956-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Stress%20 testing housestaff%20didactic_10092014[1]](https://cdn.slidesharecdn.com/ss_thumbnails/stress20testinghousestaff20didactic100920141-141013101524-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)













![ivct and ivrt IN CARDIAC CYCLE [Autosaved] .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ivctandivrtautosaved-copy-250829033609-78e4fe1b-thumbnail.jpg?width=640&height=640&fit=bounds)


































