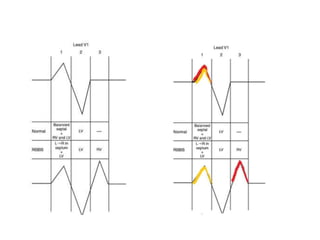
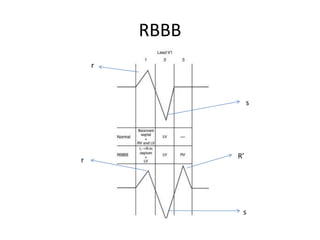
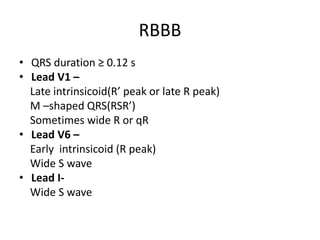
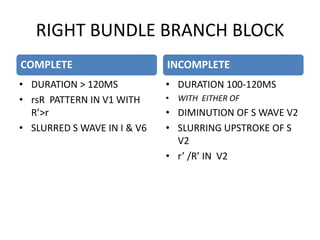
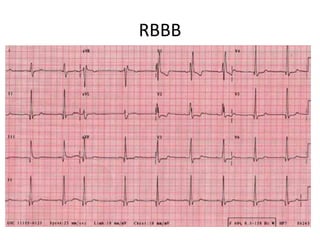
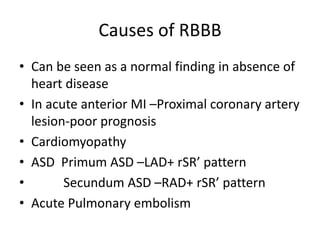
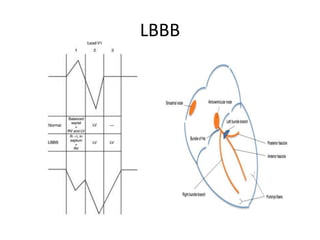
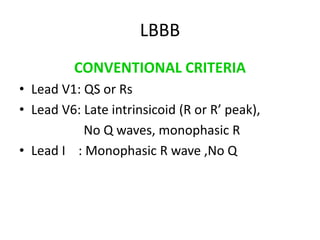
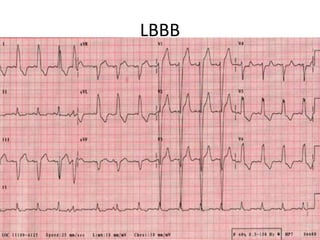
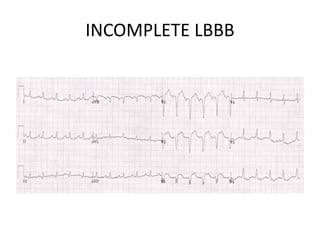
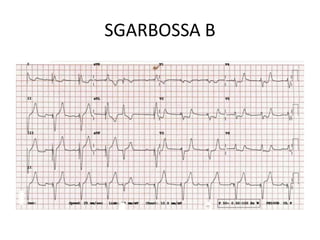
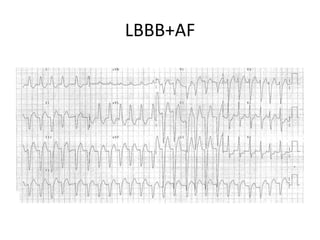
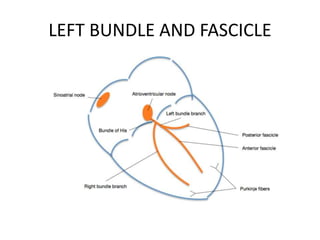
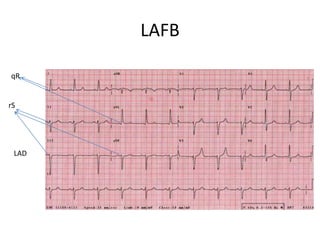
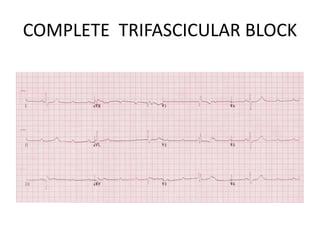
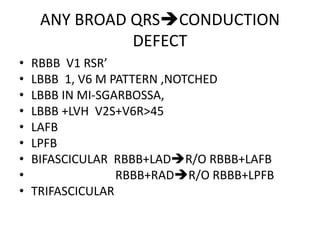
RBBB is characterized by a QRS duration ≥0.12s with an RSR' pattern in V1 and a wide S wave in V6. Causes include myocardial infarction, cardiomyopathy, and pulmonary embolism. LBBB has a QS or rS pattern in V1 and a late intrinsicoid deflection in V6. It is associated with ischemic heart disease and cardiomyopathy. New onset LBBB alone is no longer considered a STEMI equivalent. The Sgarbossa criteria help identify MI in the presence of LBBB. Left anterior and posterior fascicular blocks involve specific QRS and axis changes and help localize conduction system disease. Trifascicular block represents complete heart block with bifascicular






























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






