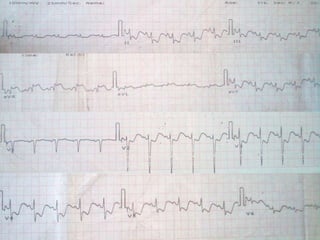
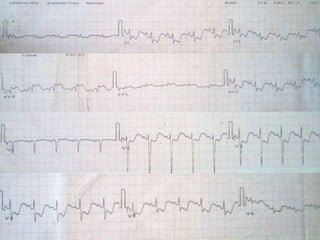
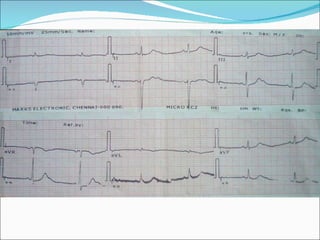
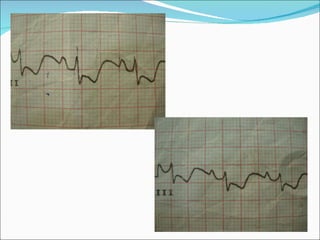
A 40-year-old male was admitted with acute watery diarrhea for 3 days and a history of recurrent diarrhea over the past 4 months. Laboratory tests found HIV positivity and hypokalemia. An ECG showed changes consistent with hypokalemia including ST depression and flattened T waves. After potassium supplementation, a repeat ECG showed normalization of potassium levels and resolution of the hypokalemia-related ECG changes.





















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















