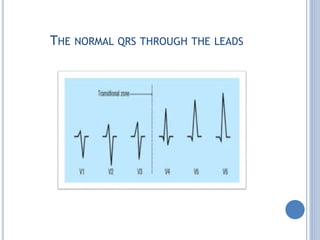
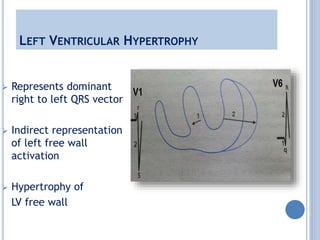
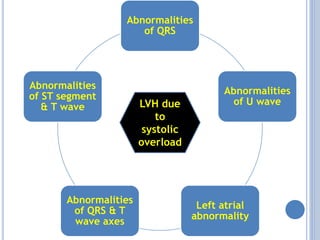
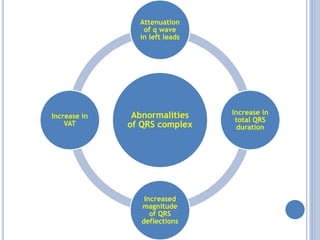
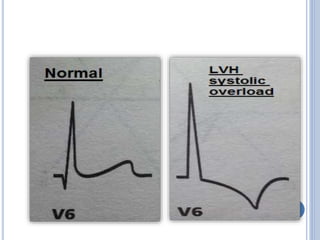
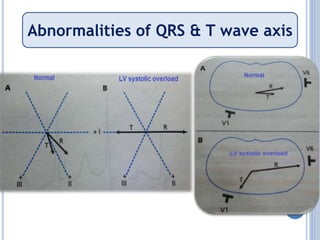
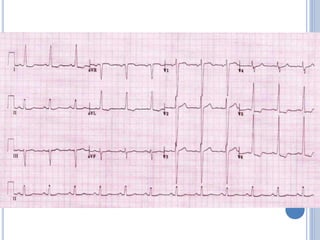
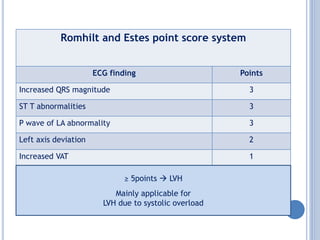
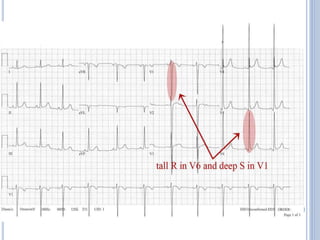
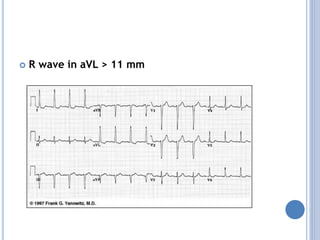
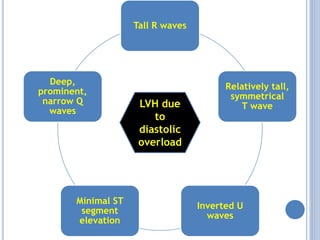
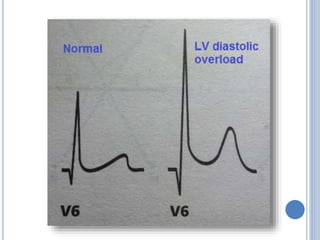
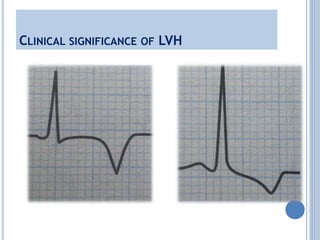
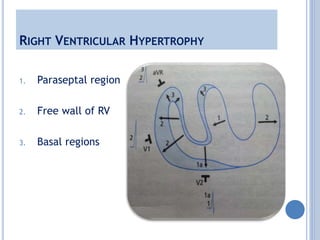
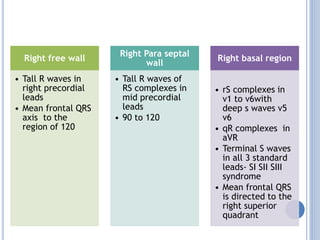
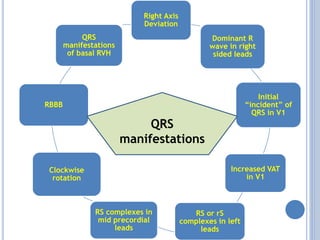
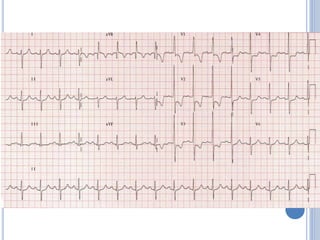
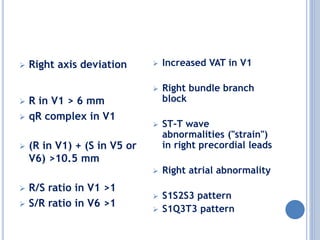
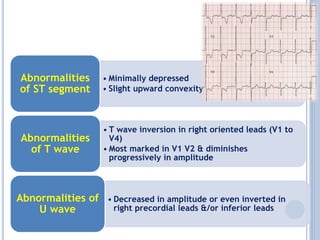
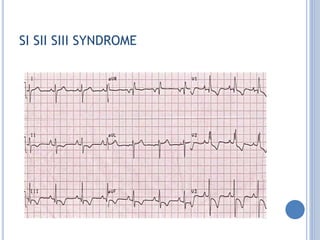
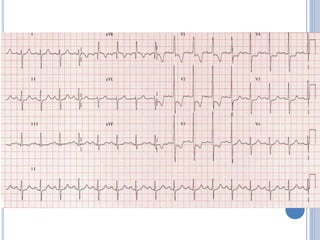
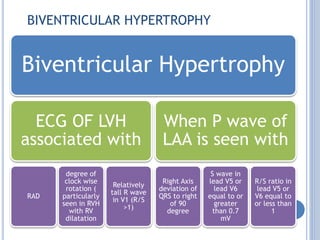
This document discusses left ventricular hypertrophy (LVH) and right ventricular hypertrophy (RVH). It defines LVH as an increase in left ventricle mass due to increased wall thickness or cavity size. There are two types of LVH - systolic overload from conditions like hypertension which compromise the left ventricle during systole, and diastolic overload from things like valvular diseases which compromise it during diastole. The document outlines ECG criteria for diagnosing LVH including Sokolov-Lyon and Cornell voltage criteria. It also discusses RVH manifestations on ECG like right axis deviation, tall R waves in right precordial leads, and an S1S2S3 pattern.