Downloaded 261 times


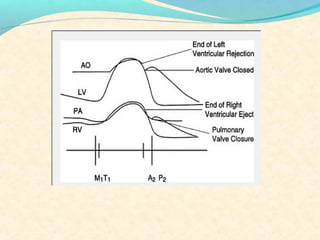
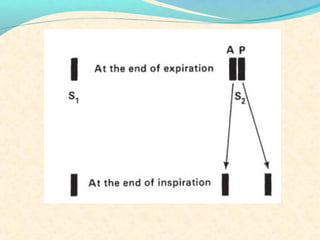
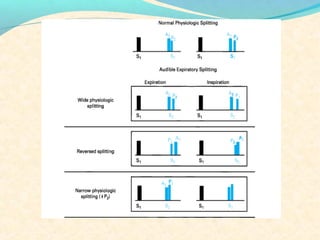
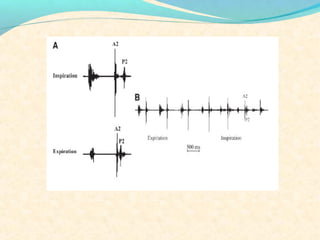

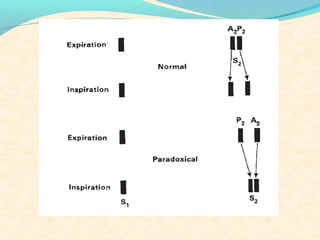
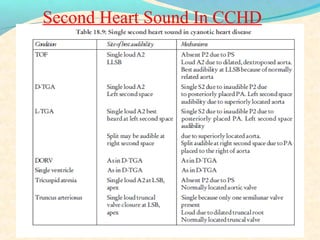
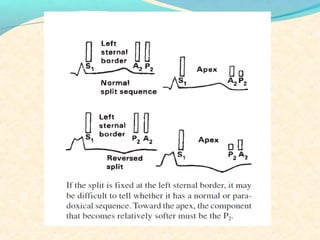
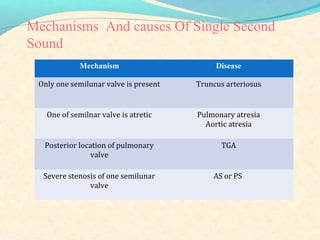
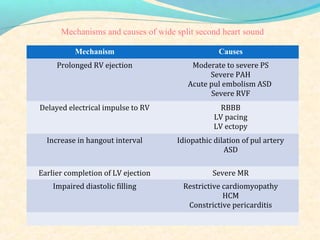
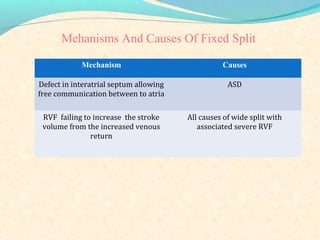
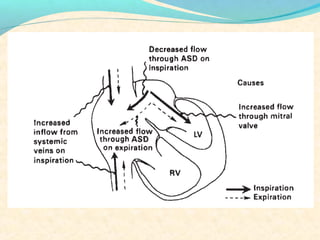
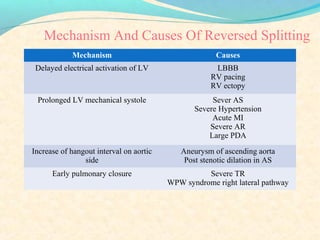
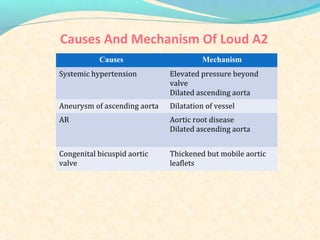
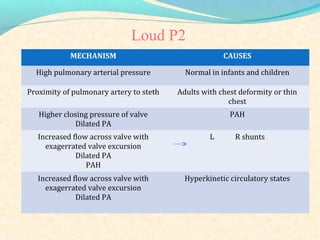
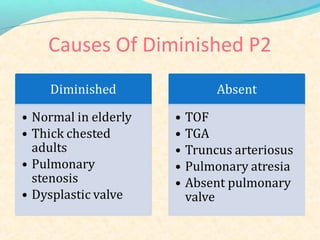
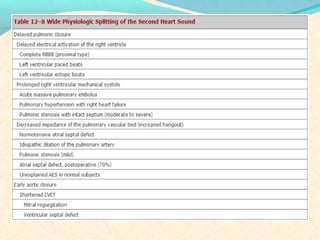
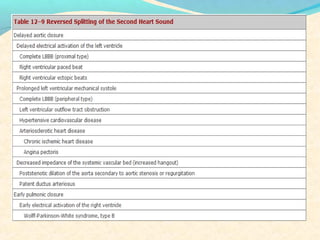
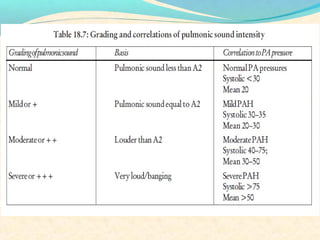
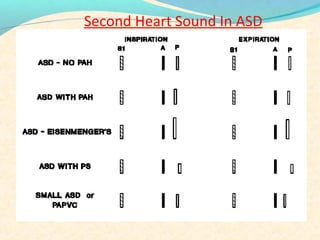
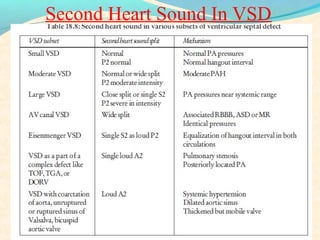
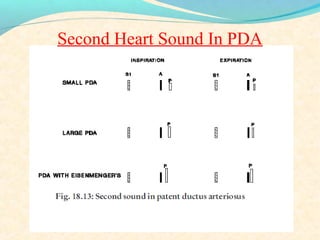
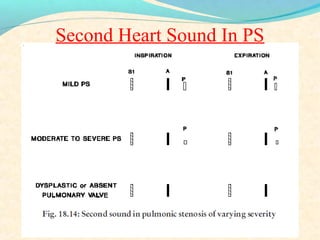
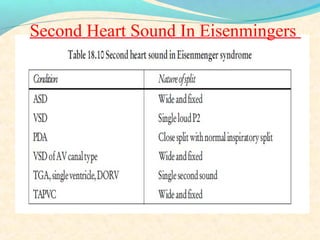
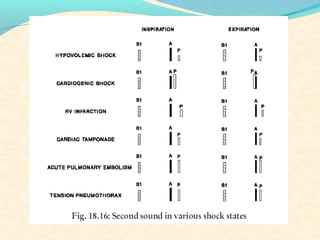

The second heart sound occurs at the end of systole due to closure of the semilunar valves. There are normally two components: A2 from aortic valve closure and P2 from pulmonary valve closure. A2 is typically louder due to higher pressures in the aorta. The components are normally split, with A2 occurring earlier due to differences in vascular resistance and compliance between the pulmonary and systemic circulations. Widening of the split may indicate conduction delays or pulmonary hypertension. Reversed or paradoxical splitting can occur in conditions that delay left ventricular ejection such as left bundle branch block. Single second heart sounds may result from fusion of the components or absence of one.
































































![[Int. med] heart murmurs from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/b29t6cwrtzwunmrfazue-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171700-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)






















