Downloaded 338 times
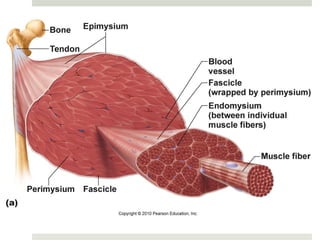
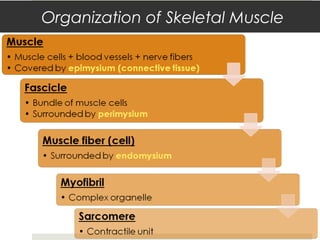
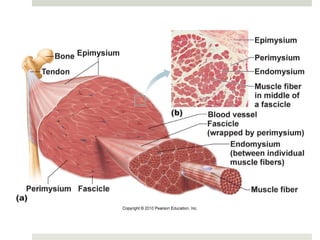
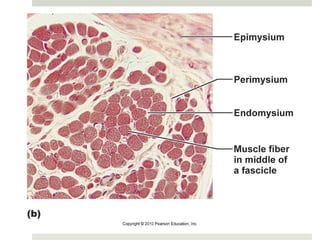
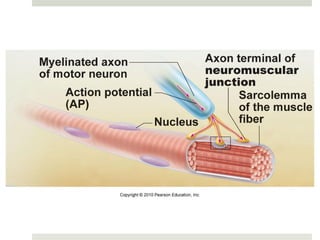
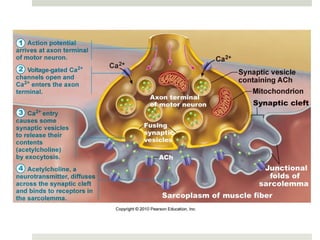
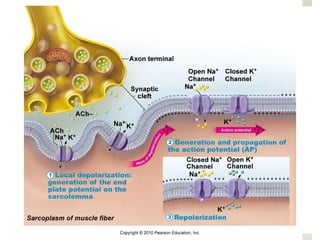
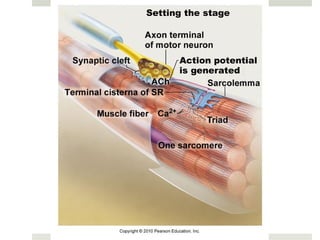
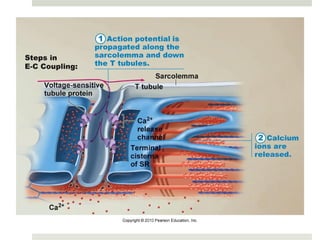
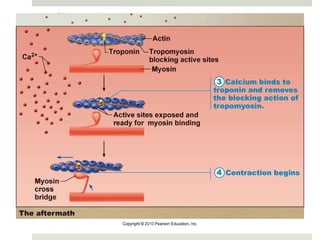
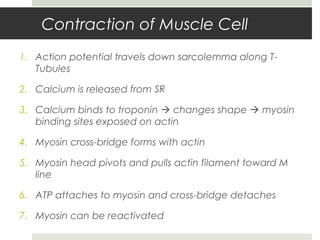
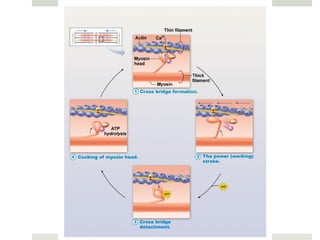


The document provides an extensive overview of muscular anatomy and physiology, detailing muscle types, structures, and functions. It discusses the processes involved in muscle contraction, the neuromuscular junction, and effects of neurotransmitters like acetylcholine. Additionally, it covers muscle responses, types of contractions, exercise impacts, and various conditions affecting muscle health.


























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















