CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx
A clinical case presentation on Subdural Hematoma (SDH) covering diagnosis, investigations, treatment, surgical management, and pharmacist interventions.
Patient demographic data:-
NAMEOF PATIENT: Modiyam Adhi
Reddy
S/O : M. Narayana Reddy
Age: 74 years
Gender: Male
Department:- Neurosurgery
Date of admission:7/6/23
Martial status: Married
Blood group: “B” Positive
3.
Subjective
evidence:-
Reasons for admission:- pt is alleged to have injury due to
Self fall from Home at of 5:30 AM on 07/06/23 at Home.
Present illness:-
c/o- Head injury
.
Nose bleed from Right nostril.
Epilepsy,
no vomiting.
Previous Illness:-
k/c/o Bronchial asthma.Pt is on medication.
No H/O of HTN,DM,TB.
ASSESMENT:
Based on MRI
Theappearance of a haematoma varies with the biochemical
state of haemoglobin which varies with the age of the
haematoma.
The classic appearance of an acute subdural haematoma is a
crescent shaped homogeneously hyperdense extra axial
collection.
Isodense due to low HB .
Diagnosis – B/L unilateral frontotemporoparietal [FTP] chronic
SDH [Sub Dural Haematoma].
7.
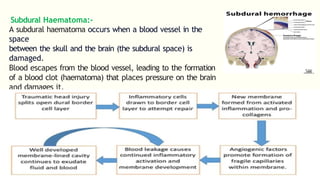
Subdural Haematoma:-
A subduralhaematoma occurs when a blood vessel in the
space
between the skull and the brain (the subdural space) is
damaged.
Blood escapes from the blood vessel, leading to the formation
of a blood clot (haematoma) that places pressure on the brain
and damages it.
Pathophysiology:-
9.
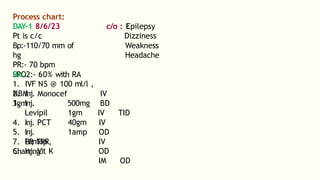
c/o : Epilepsy
Dizziness
Weakness
Headache
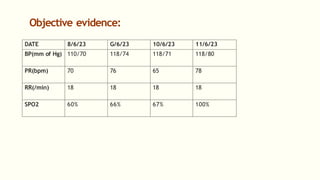
Processchart:
DAY-1 8/6/23
Pt is c/c
Bp:-110/70 mm of
hg
PR:- 70 bpm
SPO2:- 60% with RA
Rx :-
1. IVF NS @ 100 ml/l ,
NBM
2. Inj. Monocef
1gm
3. Inj.
Levipil
4. Inj. PCT
5. Inj.
Pantop
6. Inj. Vit K
500mg
1gm
40gm
1amp
IV
BD
IV TID
IV
OD
IV
OD
IM OD
7. BP
, TPR,
Charting.
10.
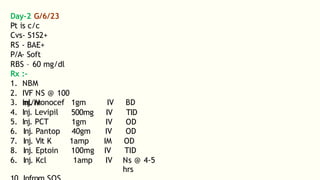
Day-2 G/6/23
Pt isc/c
Cvs- S1S2+
RS - BAE+
P/A- Soft
RBS – 60 mg/dl
Rx :-
1. NBM
2. IVF NS @ 100
ml/hr
3. Inj. Monocef
4. Inj. Levipil
5. Inj. PCT
1gm
500mg
1gm
IV
IV
IV
BD
TID
OD
6. Inj. Pantop 40gm IV OD
7. Inj. Vit K 1amp IM OD
8. Inj. Eptoin 100mg IV TID
6. Inj. Kcl 1amp IV Ns @ 4-5
hrs
11.
Day-3 10/6/23
Blood Transfusionis Done
Pre transfusion details-
BP - 110/80 mm of hg
PR - 78 bpm
SpO2 – 100%
Temp-68.4 F
Post transfusion details-
Bp- 112/84 mm of
hg PR – 80 bpm
SpO2- 100%
Temp- 68.4 F
Intra-Op:-
Uneventful
1 RL
1.IVF
1 NS
2.Inj.Dexmedetomi
12.
Past- Op :-
Ptis c/c
Bp- 118/72 mm of hg
PR-
66/min
CVS- S1S2+
RS-BAE+
Advice:-
1.NBM till
Further
Order
2.Head end
elevation
3. O2
inhalation
@
4L/hrs
4.Consider
13.
Operation Notes :-
AnaesthesiaNotes:
Sx-B/L FTP Burrhole evacuation decresed scalp
block.
Pre-OP:-
Pt is c/cGc-Fair (Glasgow coma)
BP-123/70 mm of hg
PR- 82/min
Cvs- S1S2+
RS-BAE+
Procedure:-
Using 15ml of 0.25% Bupivacaine.
15ml of 2% Lignocaine.
10 ml of distilled Water.
Added with 30 µ dexmedetomidine
14.
B/L Supra-Orbtial -3ml of drug is injected.
Supra –Trochleae - 3ml of drug is
injected. Zygomatico Temporal - 3ml of drug
is injected. Auriculo Temporal - 3ml of drug
is injected.
Greater Occipital - 3ml of drug is injected.
Lesser Occipital – 2-3ml of drug is
injected.
B/L Scalp block is done . Adequate
analgesia achieved. Surgery proceeded.
15.
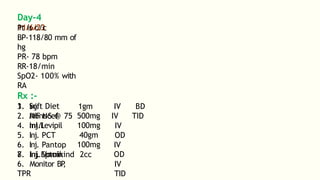
Day-4
11/6/23
Pt is c/c
BP-118/80mm of
hg
PR- 78 bpm
RR-18/min
SpO2- 100% with
RA
Rx :-
1. Soft Diet
2. IVF NS @ 75
ml/l
1gm
3. Inj.
Monocef
4. Inj.Levipil
5. Inj. PCT
6. Inj. Pantop
7. Inj.Eptoin
500mg
100mg
40gm
100mg
8. Inj. Vomikind 2cc
IV BD
IV TID
IV
OD
IV
OD
IV
TID
6. Monitor BP
,
TPR
16.
Day-5 12/6/23
Pt isc/c
BP-118/71mm of
hg PR-82 bpm
RR-18/min
SpO2- 64% with
RA
Physical Rx :-
I. Ankle pumps advised to prevent
DVT
.
II. Breathing excises are advised.
III. Pt made to sit.
Rx :
-
1. Soft Diet
2. IVF NS @ 75
ml/l 1gm
3. Inj.
Monocef
4. Inj.Levipil
5. Inj. PCT
6. Inj. Pantop
7. Inj.Eptoin
8. Inj.
Vomikind
500mg
100mg
40gm
100mg
2cc
IV BD
IV TID
IV
OD
IV
OD
IV
TID
IV
6. Monitor BP
,
TPR
10. Infrom SOS
17.
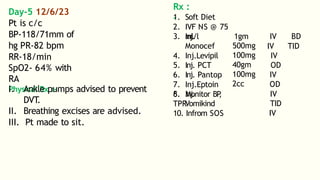
S.No Brand NameGeneric Name Indication Dose Frequency ROA
1. Inj. Monocef Ceftriaxone It is used to treat
bacterial
infections.
1gm BD IV
2. Inj. Levipil Levetiracetam used to treat seizures
(fits) in epilepsy
500mg TID IV
3. Inj. PCT Acetaminophen used to relieve pain 100mg OD IV
4. Inj. Mephyton vit k Helps blood to clot
and prevent
excessive bleeding.
1amp OD IM
5. Inj. Protonix Pantoprazole T
o treat
gastro-esophageal
reflux
40gm OD IV
6. Inj.Eptoin phenytoin used to treat
and prevent
100mg TID IV
PLANNING :
-
18.
Pharmacist Intervention :-
Concurrent use of PCT and Eptoin may result in
decreased PCT effectiveness and an increased risk
of hepatotoxicity.
Eptoin (Phenytoin) and Levetiracetam: Phenytoin may
decrease Levetiracetam's efficacy; monitor seizure
control.
Eptoin (Phenytoin) and Monocef (Ceftriaxone):
Phenytoin may decrease Ceftriaxone's efficacy due
to altered liver enzyme activity
.
19.
Patient Counselling :-
Ensure to get plenty of sleep upto symptoms.
Be involved is your treatment.
How to take medications.
Possible medications or dietery interactions.
Special monitoring requirement for eg- Blood
test.
Minimize stress.
Improve air quality in room and practice
good hygiene .

![•HbsAg: Negative
•HIV: Non-reactive
•HCV: Non-reactive
Electrolytes:
Na+ : 135.4
mMol/L K+ : 3.43
mMol/L cl- :
100.2 mMol/L
Ionized Ca2+ :
4.75 mg/dl
Haemoglobin :
[N- 135-155]
[N- 3.5-5.5]
[N- 68-
107] [N-
4.8-5.6]
[N-13-16
g/dl]](https://image.slidesharecdn.com/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375/85/CASE_PRESENTATION_ON_subdural_hematoma-SDH-1-FINAL-PPT-1-pptx-5-320.jpg)
![ASSESMENT:
Based on MRI
The appearance of a haematoma varies with the biochemical
state of haemoglobin which varies with the age of the
haematoma.
The classic appearance of an acute subdural haematoma is a
crescent shaped homogeneously hyperdense extra axial
collection.
Isodense due to low HB .
Diagnosis – B/L unilateral frontotemporoparietal [FTP] chronic
SDH [Sub Dural Haematoma].](https://image.slidesharecdn.com/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375/85/CASE_PRESENTATION_ON_subdural_hematoma-SDH-1-FINAL-PPT-1-pptx-6-320.jpg)
![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://image.slidesharecdn.com/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375/85/CASE_PRESENTATION_ON_subdural_hematoma-SDH-1-FINAL-PPT-1-pptx-20-320.jpg)






























![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















