Downloaded 803 times
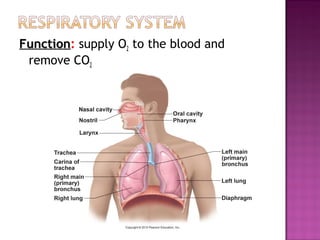
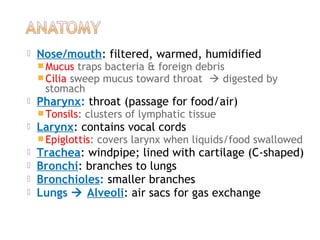
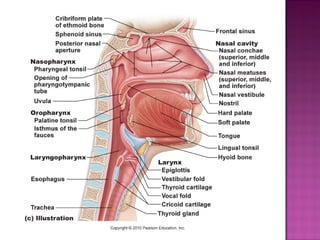
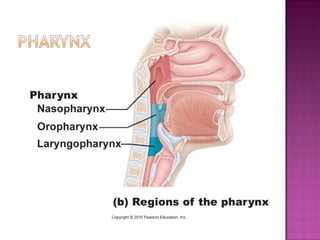
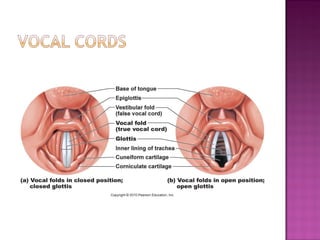
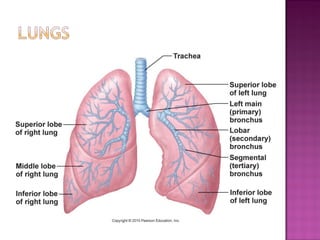
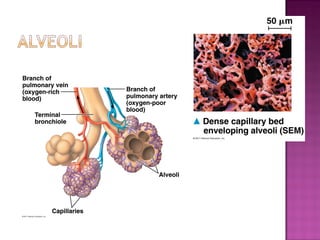
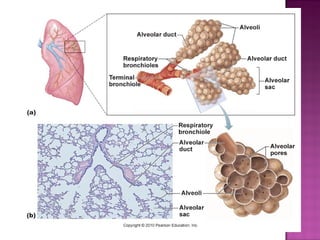
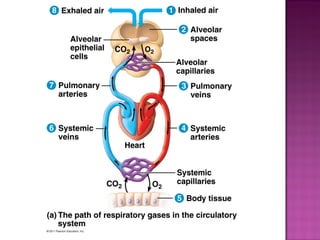
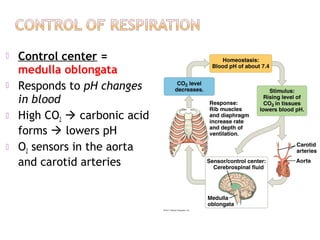
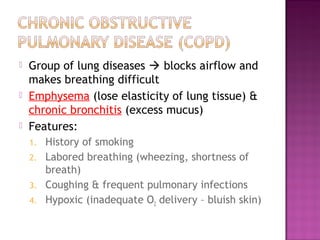
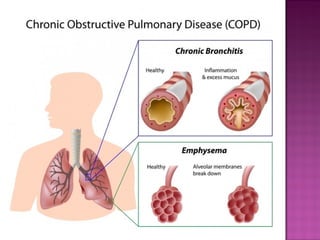
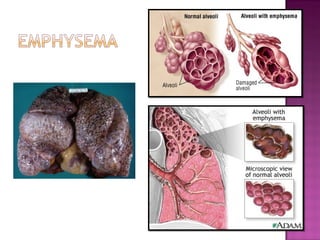
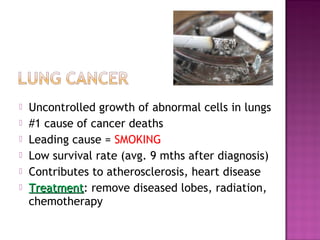
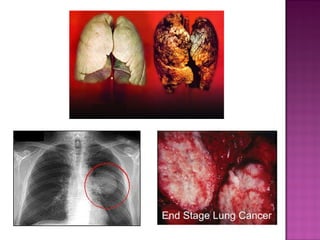

The document outlines the organs of the respiratory passageway, detailing the functions and mechanics of breathing, including the roles of various muscles and lung capacities. It discusses conditions affecting respiratory health such as emphysema, chronic bronchitis, asthma, and pneumonia, highlighting their causes, symptoms, and treatments. Additionally, it emphasizes the importance of oxygen and carbon dioxide transport in the blood, alongside the impact of lung diseases on overall health.










































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)