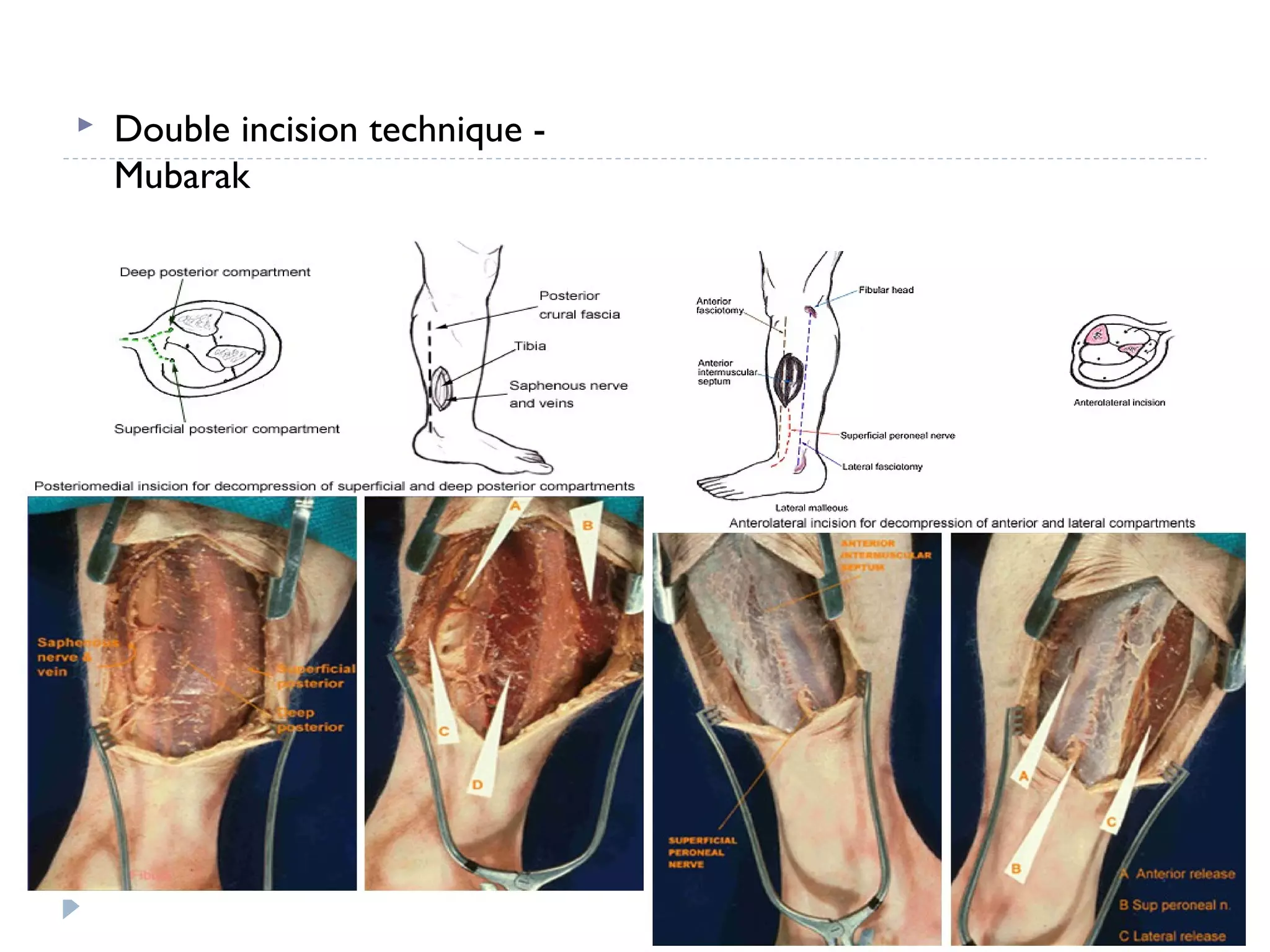
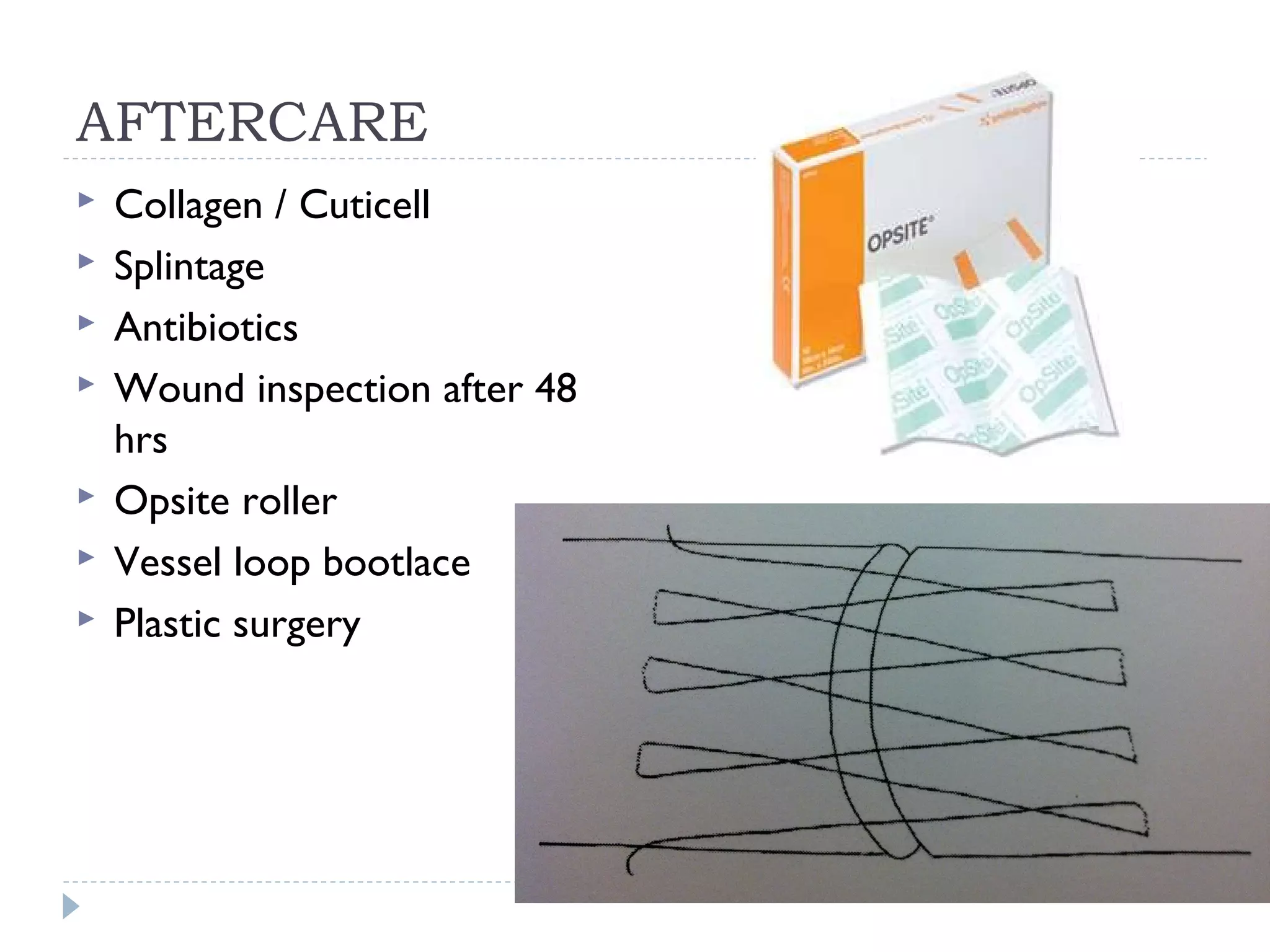
Acute compartment syndrome is caused by increased pressure within the confined space of a muscle compartment, restricting blood flow and often resulting from trauma such as fractures or crush injuries. Diagnosis involves assessing disproportionate pain and pressure measurements. Treatment involves surgical fasciotomy to release the fascia and decompress the compartment if pressure is within 30 mmHg of diastolic or above 45 mmHg. Proper wound care after fasciotomy and stabilization of any fractures is needed to prevent complications like contracture, infection, and paralysis.