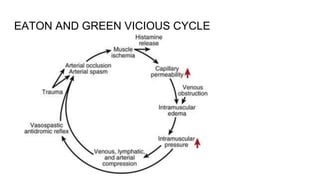
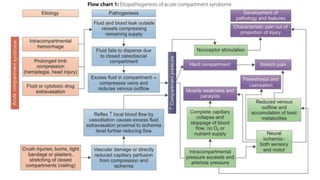
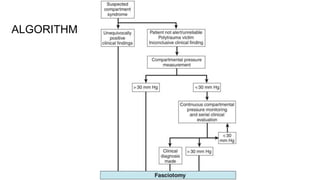
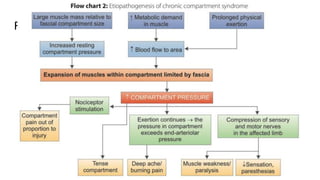
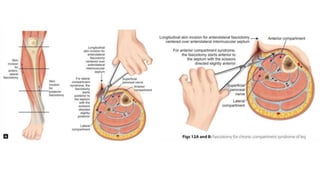
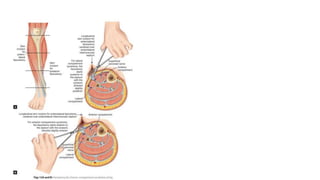
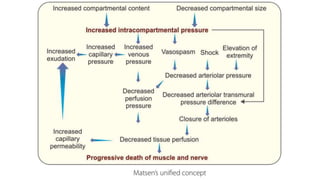
Compartment syndrome occurs when increased pressure within the osteofascial compartments of the body impairs blood flow. It is a surgical emergency. The document discusses compartment syndrome including definition, types, anatomy, pathophysiology, etiology, clinical evaluation, diagnosis using compartment pressure measurement, and management through fasciotomy to release pressure if indicated. Early diagnosis and fasciotomy before permanent nerve and muscle damage occurs are important to prevent complications.