Downloaded 334 times


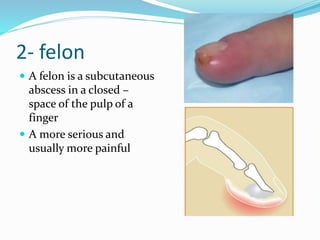


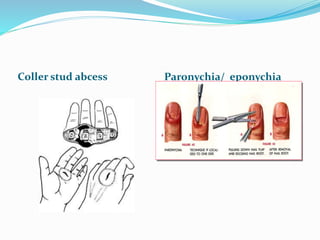


The document discusses hand infections, covering relevant anatomy, pathogenesis, types of infections, and treatment management. Common bacterial and fungal pathogens are noted, along with specific infections like paronychia, felon, and flexor tenosynovitis. The importance of early diagnosis and surgical intervention is emphasized to prevent complications and preserve hand function.





















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



