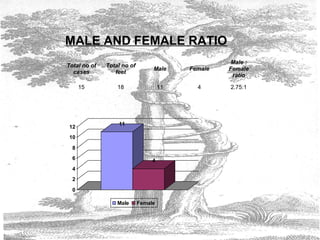
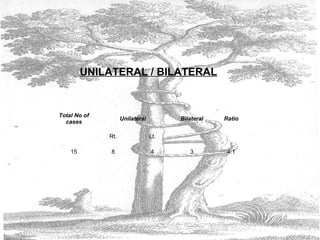
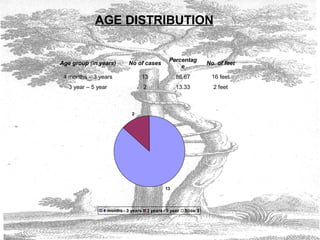
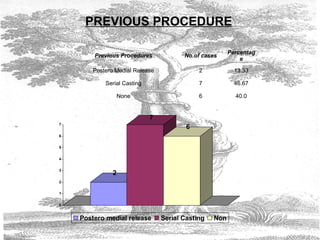
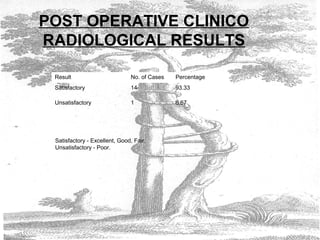
The document discusses the use of the Jess external fixator for treating recurrent, resistant, and neglected clubfoot deformities. It summarizes a study of 15 patients (18 feet) treated using this method. The results were generally good, with 14 cases rated as satisfactory and only 1 as unsatisfactory. Younger age at treatment and less severe deformities were associated with better outcomes. Complications were minor and manageable. The study concludes that Jess external fixation is an excellent technique for difficult clubfoot cases, especially when performed at an early age.