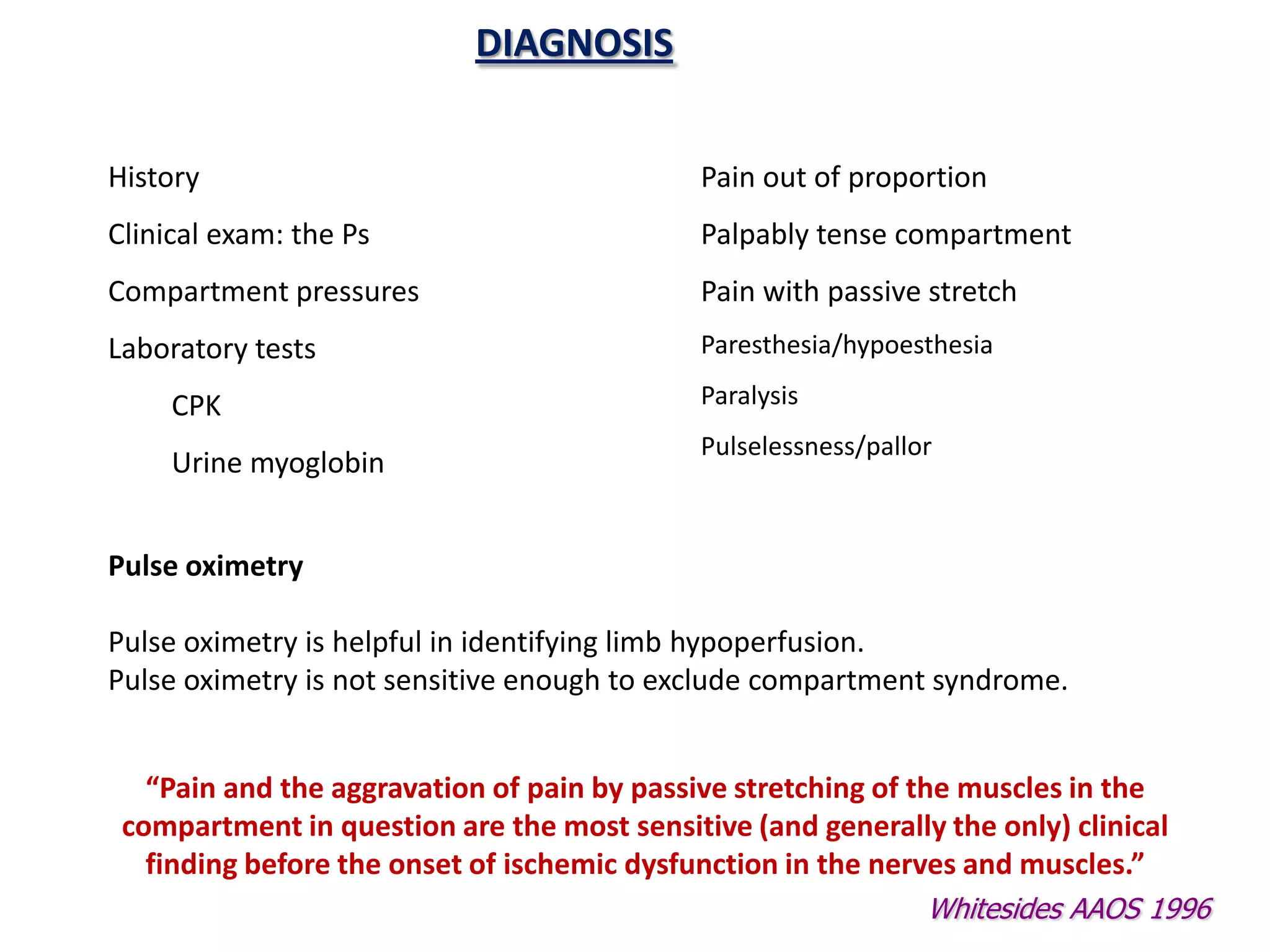










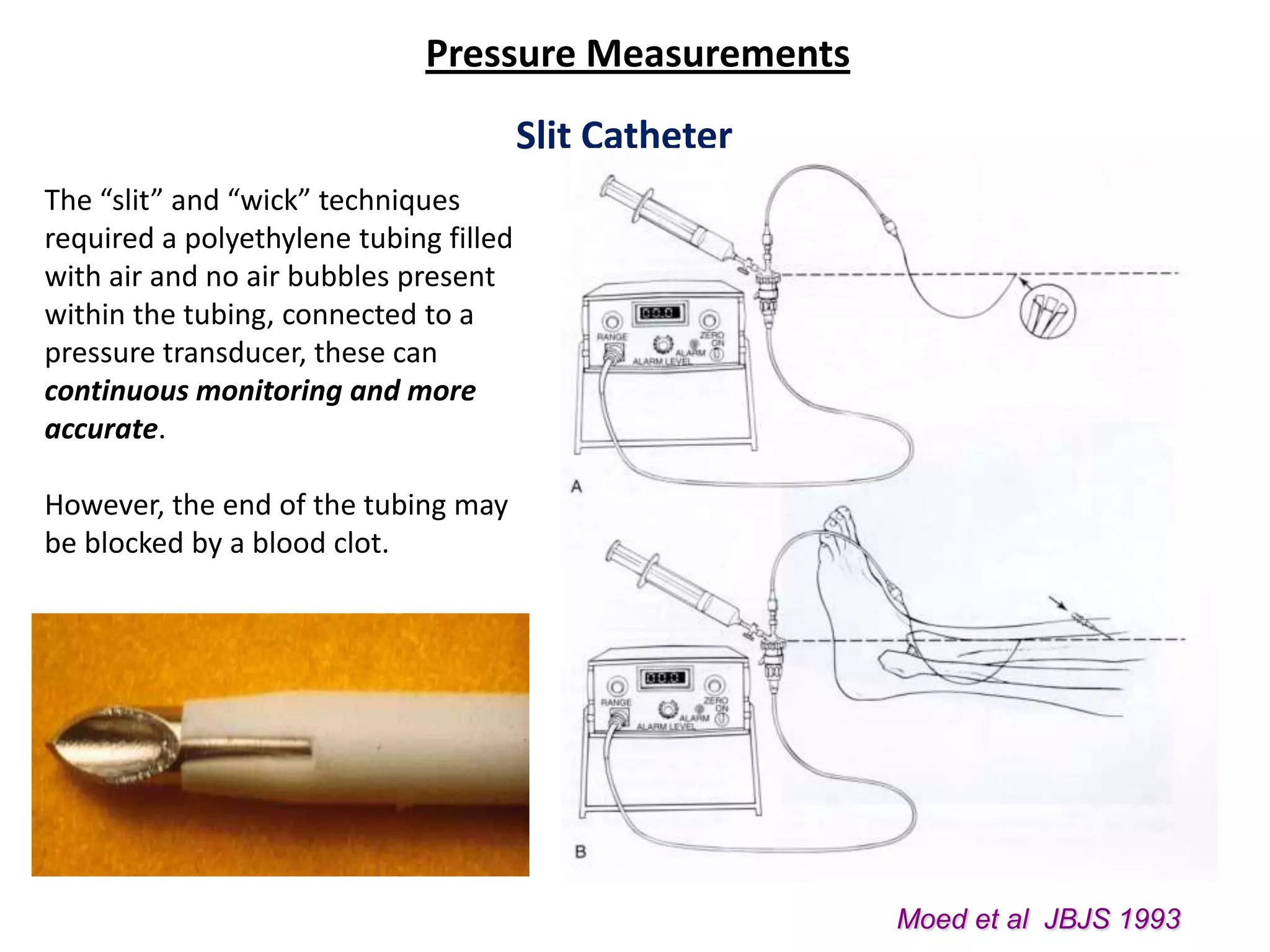
















































This document discusses compartment syndrome, beginning with a definition and classification. It then covers the history of compartment syndrome, notable contributors, and key events in understanding the condition. Etiology, incidence rates, effects of patient positioning, traction, and intramedullary nailing are examined. The pathophysiology and timeline of tissue damage are described. Diagnosis is discussed, highlighting indicators such as pain, tense compartments, pressure measurements, and laboratory tests. Clinical parameters like pain, paresthesia, paralysis and pallor are also outlined. The document emphasizes that pain, especially with passive stretching, is the most important sign and should not be waited on before intervention.