Downloaded 12 times







































































![References
• Campbell’s Operative Orthopaedics 4th Edition
• J. Maheshwari 5th Edition
• Apley’s 9th Edition
• UpToDate Version 3.0
• Torlincasi AM, Lopez RA, Waseem M. Acute Compartment Syndrome.
[Updated 2021 Feb 10]. In: StatPearls [Internet]. Treasure Island (FL):
StatPearls Publishing; 2021 Jan-. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK448124/](https://image.slidesharecdn.com/compartmentsyndrome-210930140729/75/Compartment-syndrome-77-2048.jpg)


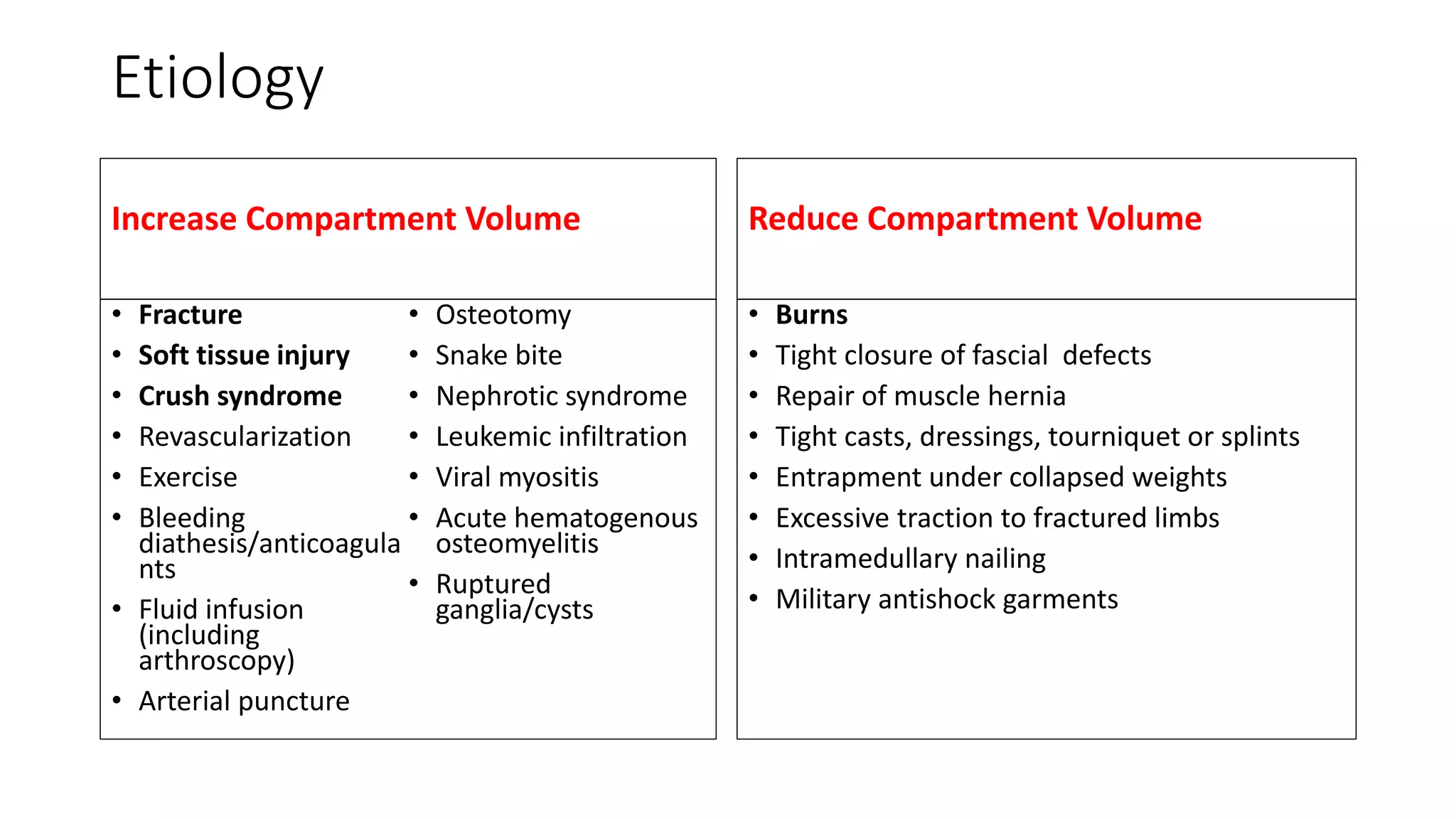
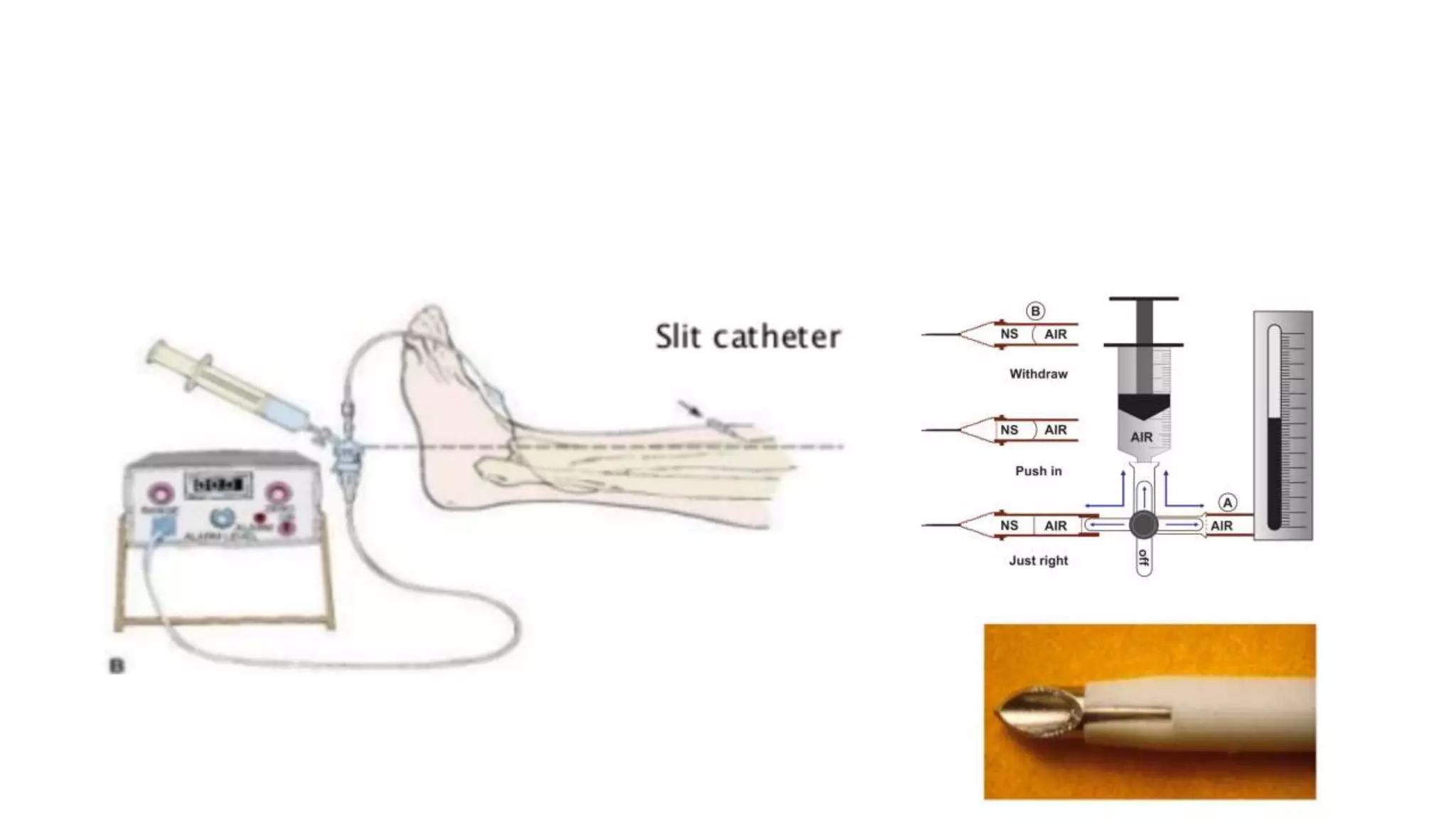
This document provides an overview of compartment syndrome, including: - It defines compartment syndrome as elevated pressure within a closed osteofascial compartment compromising microcirculation. - The most common causes are tibial fractures and soft tissue injuries. - Clinical diagnosis is based on history, exam findings like pain out of proportion, and potentially measuring compartment pressure. - Treatment is urgent fasciotomy within 6 hours for decompression if pressure is over 30mmHg. - Goals after fasciotomy are wound care, rehabilitation, and skin grafting to prevent complications like infection, contractures, and nerve damage.



































































