Downloaded 868 times
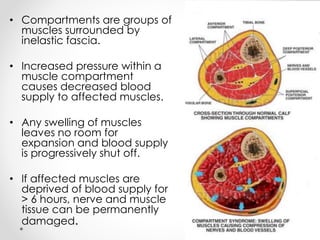
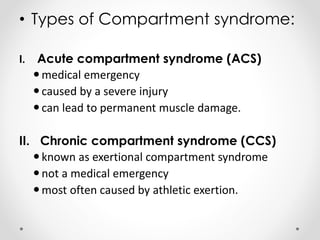


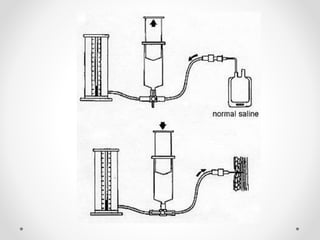
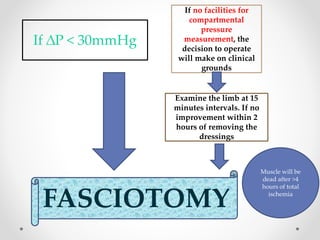



Compartment syndrome occurs when increased pressure within a muscle compartment reduces blood supply, potentially leading to permanent muscle and nerve damage if untreated for over 6 hours. It can be acute, often due to severe injuries, or chronic, typically linked to athletic exertion, with symptoms including severe pain, swelling, and loss of function. Management involves timely diagnosis and intervention, including fasciotomy in severe cases, and both non-operative and operative strategies depending on the severity of the condition.



































































