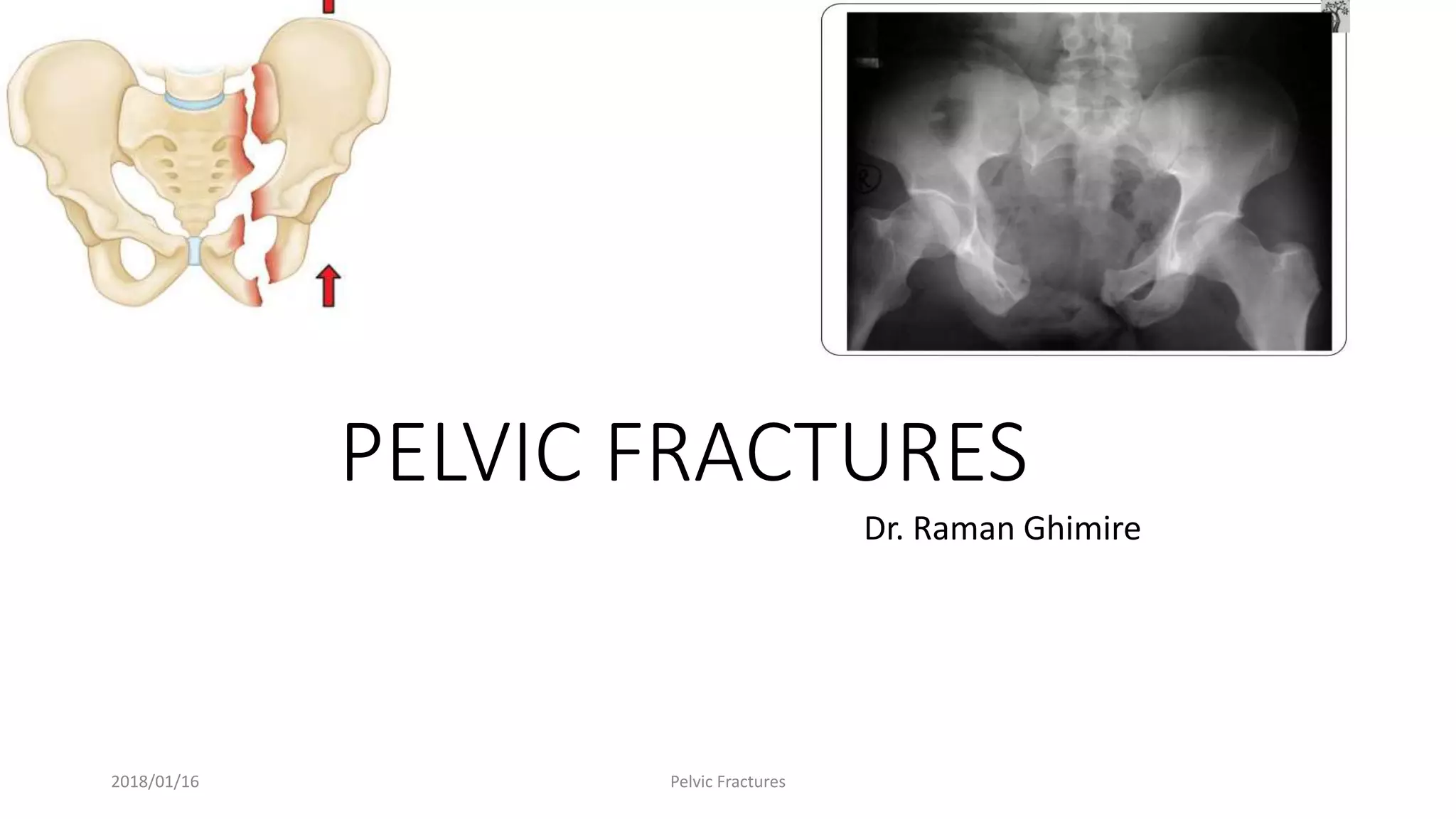
The document discusses pelvic fractures, including:
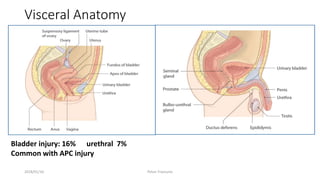
- Pelvic fractures can range from benign to life-threatening and are often associated with other injuries.
- They are commonly caused by high-energy blunt trauma like motor vehicle accidents.
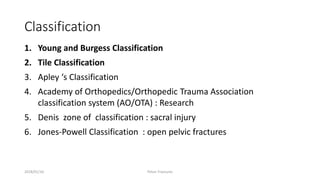
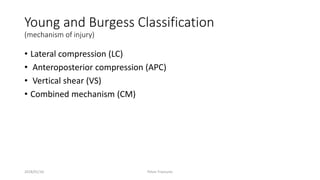
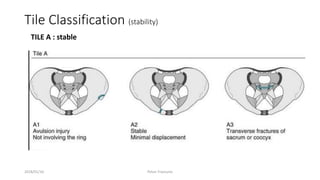
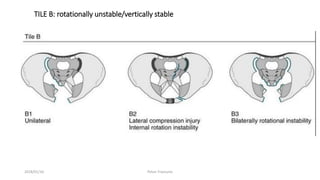
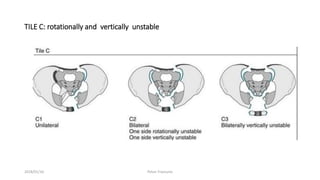
- Classification systems include the Young and Burgess system (based on mechanism of injury) and the Tile system (based on stability).
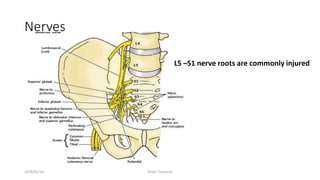
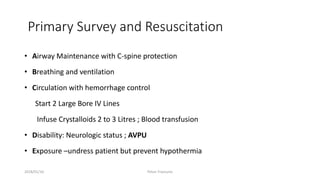
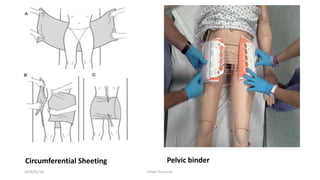
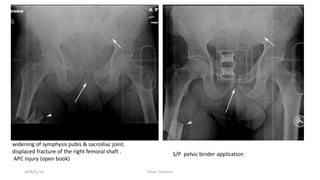
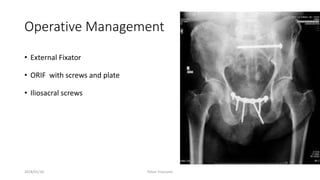
- Treatment depends on the classification but may include hemorrhage control, pelvic binding, angiography, surgery, and fixation devices. Complications can include blood loss, nerve injury, and infection.













































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






