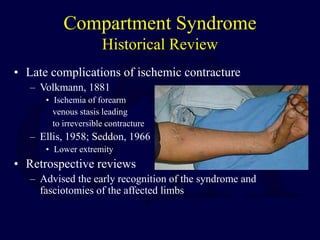
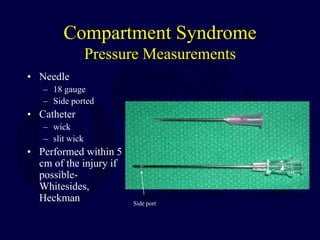
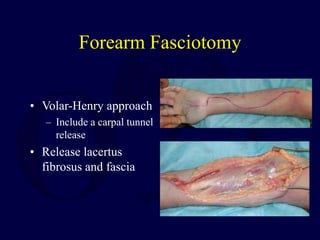
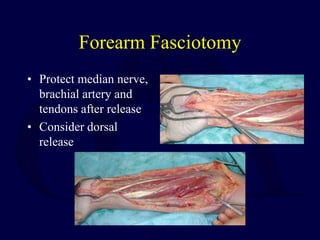
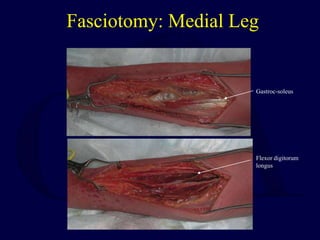
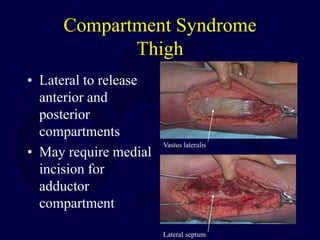
This document discusses compartment syndrome, beginning with definitions, pathogenesis, and a historical review. It then covers pathophysiology, including normal and threshold tissue pressures. Timelines for tissue survival are provided. Etiologies and diagnostic criteria are outlined. Pressure measurement techniques and indications for fasciotomy are described. Specific anatomy and approaches for fasciotomy of the forearm, leg, thigh, foot and other areas are illustrated. Post-operative care and potential medical-legal issues are also summarized.