
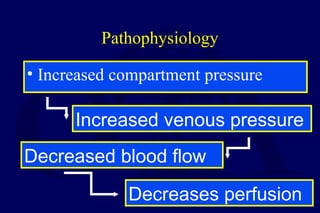
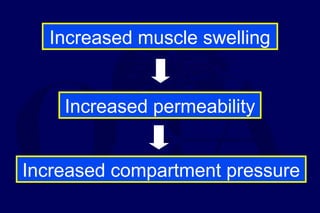
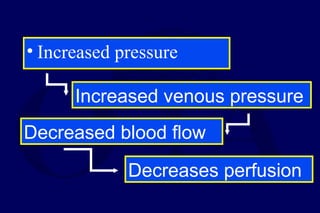
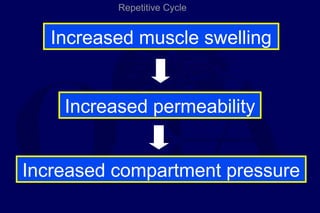
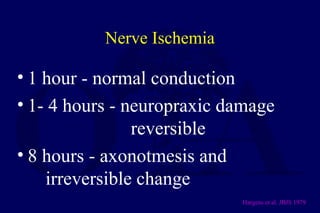
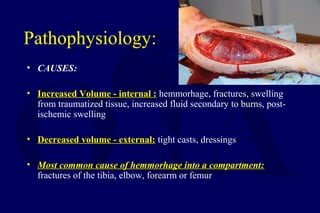

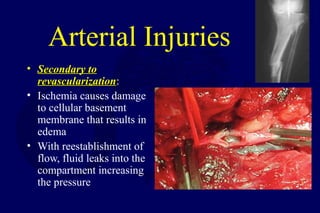





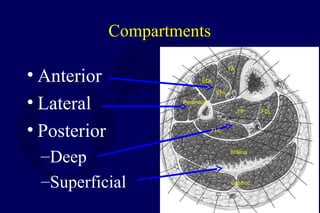


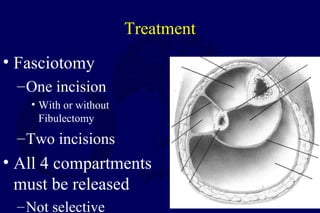
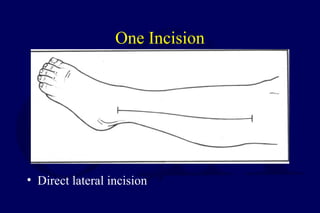



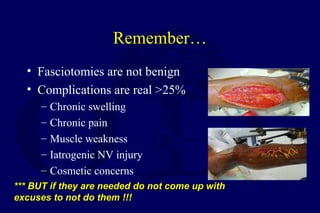


This document provides information on compartment syndromes, including: - The pathophysiology of increased pressure within closed muscle compartments leading to reduced blood flow and tissue ischemia. - Risk factors, signs and symptoms including disproportionate pain and elevated compartment pressures measured via needle technique. - Diagnosis is clinical with compartment pressures helping to confirm. - Treatment involves urgent surgical fasciotomy to decompress all affected compartments before irreversible muscle and nerve damage occurs. - Post-fasciotomy care and complications are also discussed.




































































































