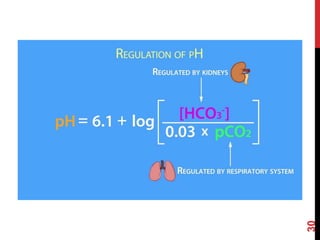
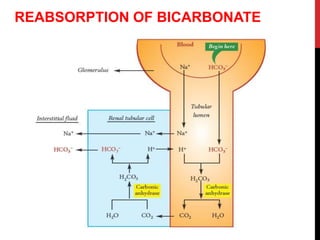
This document discusses acid-base balance and the mechanisms that regulate pH levels in the human body. It covers topics like buffers, respiratory regulation, and renal regulation of pH. The three main points are:
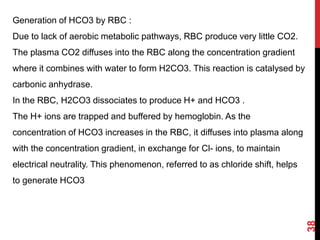
1) Buffers like bicarbonate help maintain pH levels by neutralizing excess hydrogen ions. The Henderson-Hasselbalch equation describes the buffering capacity of bicarbonate.
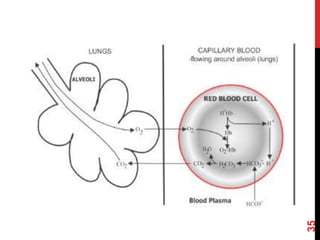
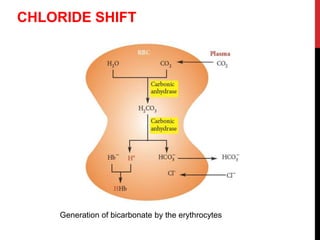
2) The respiratory system regulates pH rapidly through exhalation of carbon dioxide. Hemoglobin transports carbon dioxide as bicarbonate from tissues to the lungs.
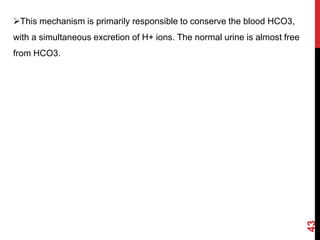
3) The kidneys regulate pH over longer periods through reabsorption of bicarbonate, and excretion of fixed acids, ammonium


![Dissociation of an acid is a freely reversible reaction. At equilibrium
the ratio between dissociated and undissociated particle is a constant.
Dissociation constant (Ka) of an acid is
[H+] [A–-]
Ka = ––––––––-
[HA]
where [H+] is the concentration of hydrogen ions, [A–] = the
concentration of anions or conjugate base, and [HA] is the
concentration of undissociated molecules.
The pH at which the acid is half ionized is called pKa of an acid
which is constant at a particular temperature and pressure.
Strong acids will have a low pKa and weak acids have a higher pKa.
Dissociation Constant](https://image.slidesharecdn.com/acid-basebalance-1-200414144745/85/Acid-base-balance-1-7-320.jpg)
![The acidity of a solution is measured by noting the hydrogen ion
concentration in the solution and obtained by the equation.
[acid] [HA]
[H+] = Ka –––––––– or ––––––
[base] [A––]
where Ka is the dissociation constant.
To make it easier, Sorensen expressed the H+ concentration as the
negative of the logarithm (logarithm to the base 10) of hydrogen ion
concentration, and is designated as the pH. Therefore,
_1_
pH = –log [H+] = log [H+]
Acidity of a Solution and pH](https://image.slidesharecdn.com/acid-basebalance-1-200414144745/85/Acid-base-balance-1-8-320.jpg)

![The relationship between pH, pKa, concentration of acid and
conjugate base (or salt) is expressed by the
Henderson-Hasselbalch equation,
[base] [salt]
pH = pKa + log ––––– or pH = pKa + log –––––
[acid] [acid]
When [base] = [acid]; then pH = pKa
Therefore, when the concentrations of base and acid are the same,
then pH is equal to pKa.
The Effect of Salt upon the Dissociation](https://image.slidesharecdn.com/acid-basebalance-1-200414144745/85/Acid-base-balance-1-11-320.jpg)













































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


