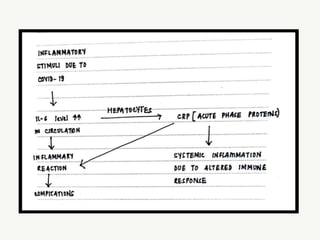
The document discusses biochemical markers associated with COVID-19, highlighting the severity and clinical relevance of various tests including d-dimer, CRP, myoglobin, IL-6, and troponin, which are critical in assessing disease progression and risk of complications. It emphasizes the impact of the second wave of COVID-19 in India, where hospitals are overwhelmed, and only a small percentage of the population has been vaccinated. Additionally, it explains the immunological and inflammatory responses triggered by the virus, which contribute to severe symptoms and potential mortality.