2
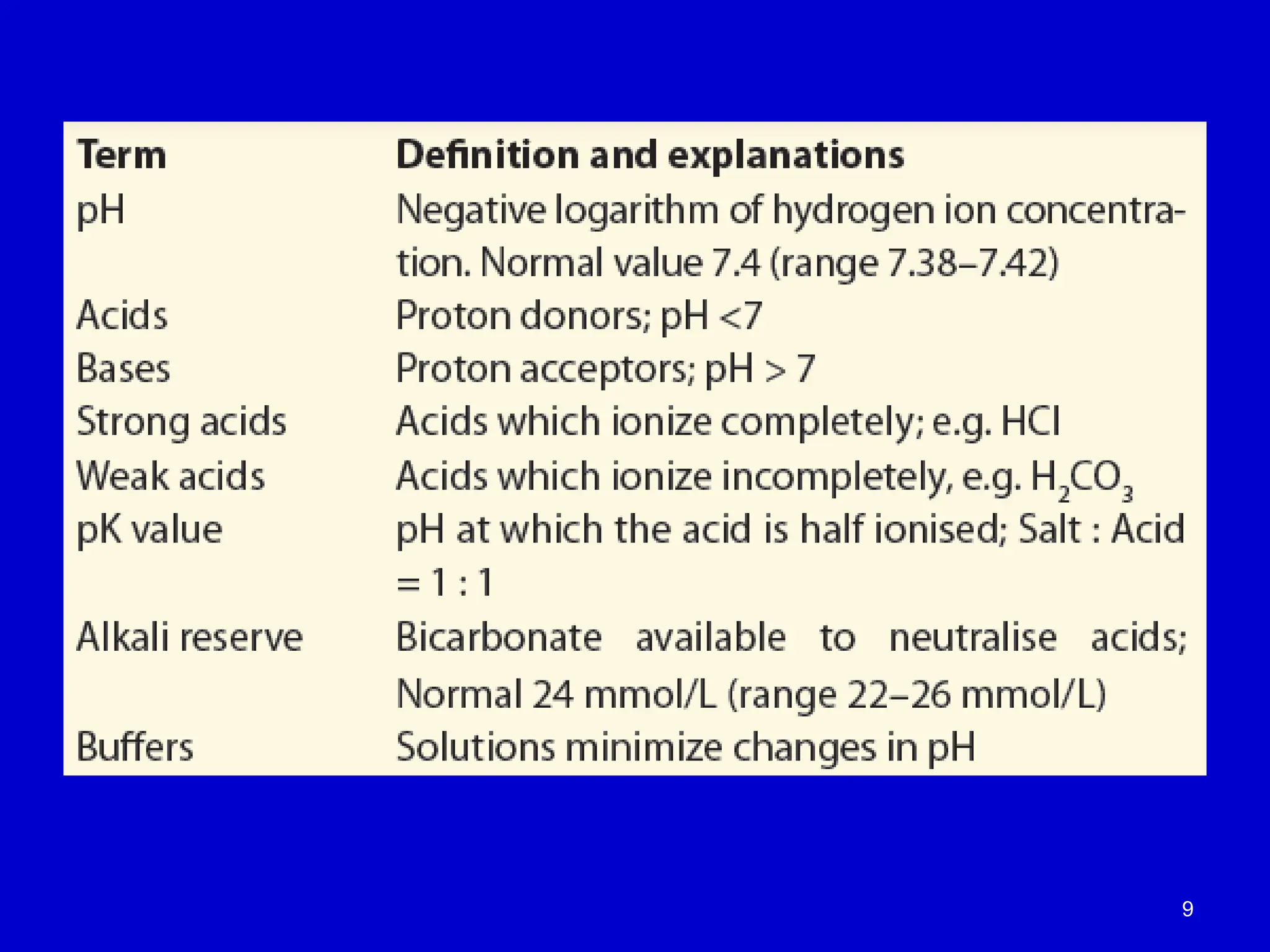
pH
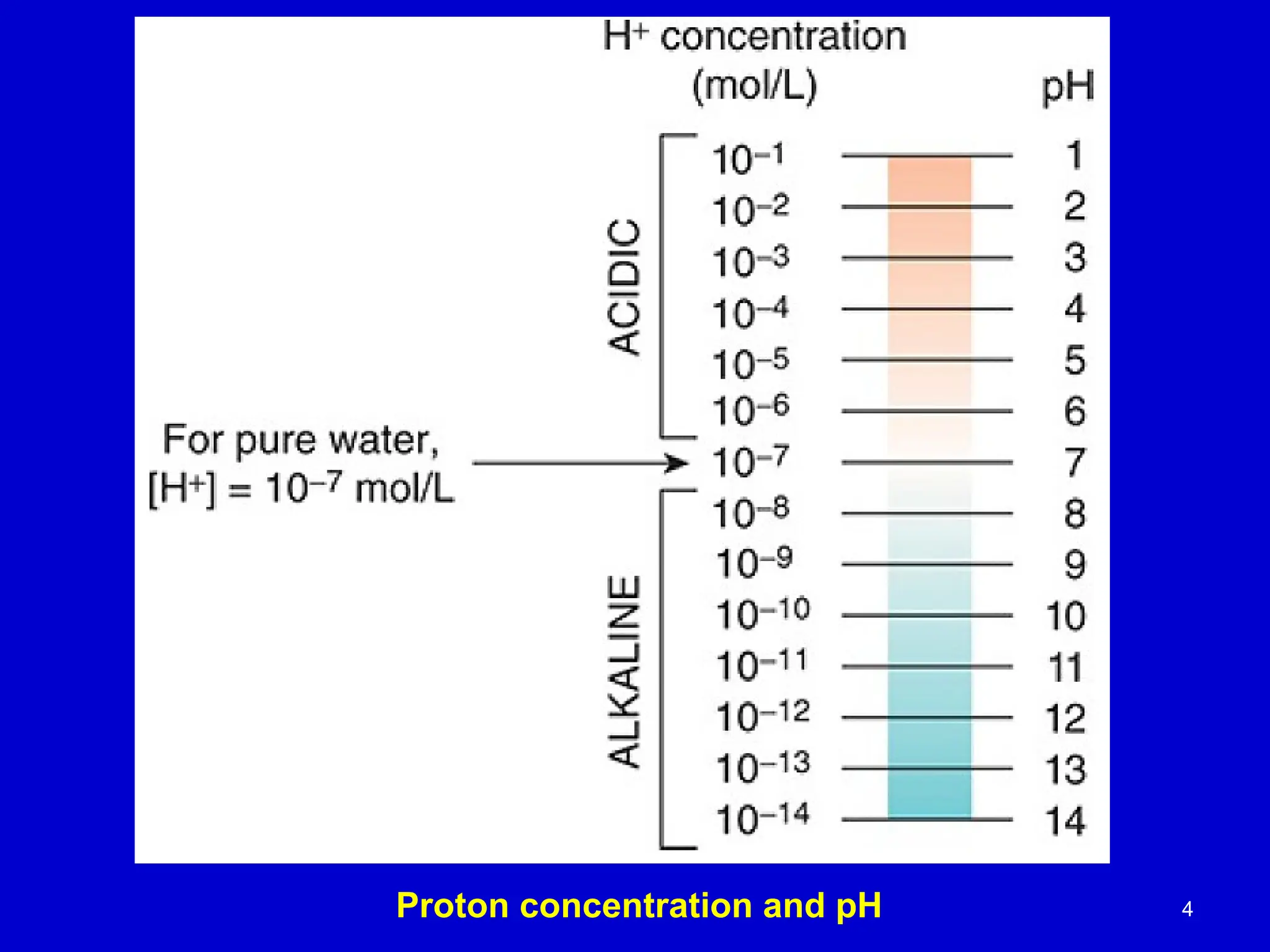
• The concentrationof hydrogen ions
determines the acidity of the solution, which
is expressed in terms of pH.
• [H+
] can be expressed as pH
• pH is negative log of [H+
]
3.
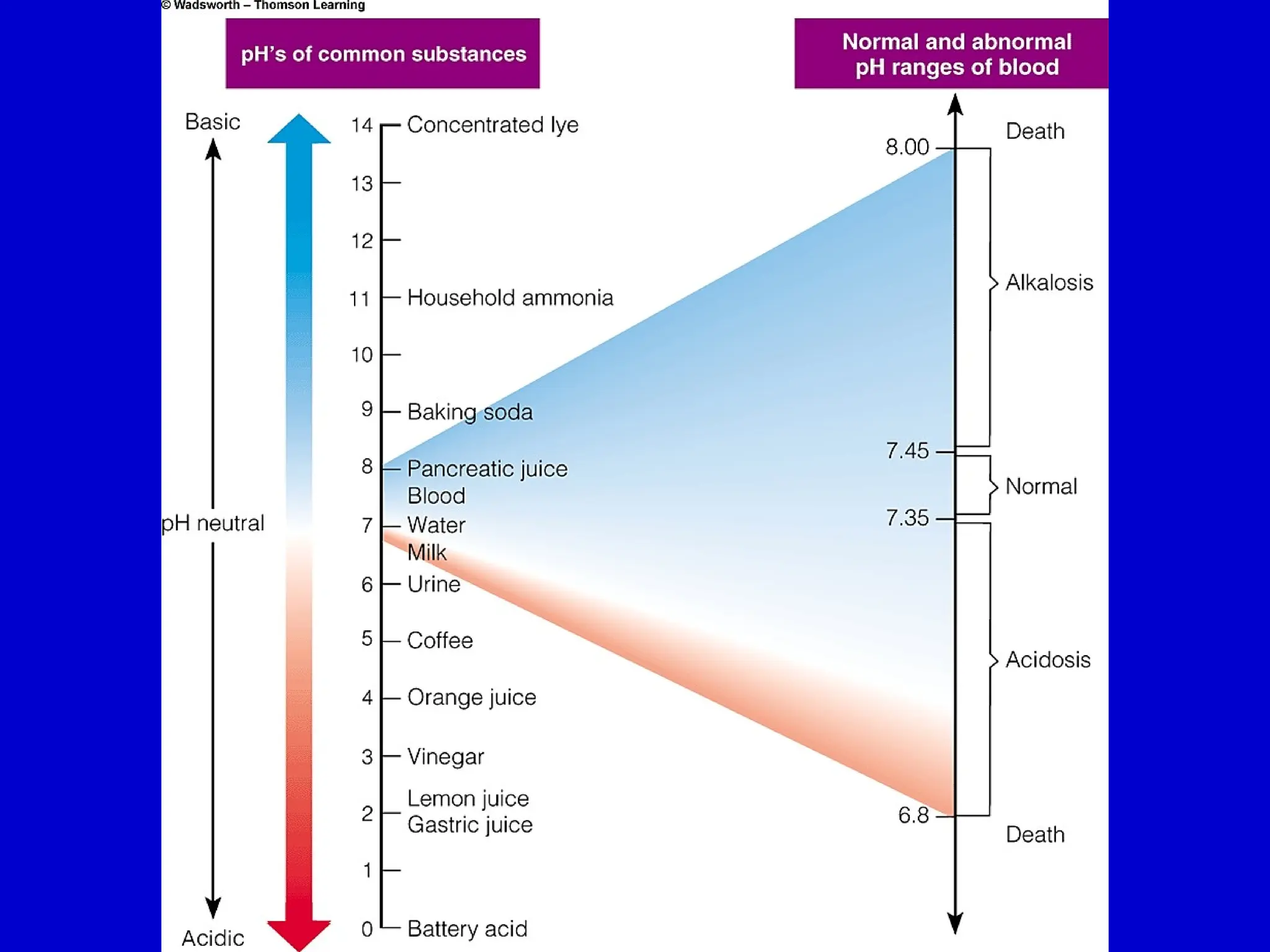
Hydrogen ion concentration
•Blood [H+
] is maintained within tight limits
– Reference values 35-45 nmol/L
– Values > 120 nmol/L or < 20 nmol/L are incompatible
with life
3
The pH Scale
Understandingthe Ion Product of Water
and the pH Scale
•Ion Product of Water (K )
ᴡ :
• K = [H ][OH ]
ᴡ ⁺ ⁻
• Basis for defining the pH scale
•Definition of pH:
• pH = –log[H ]
⁺
• Measures the concentration of
hydrogen ions in a solution
•Neutral Solutions:
• [H ] = [OH ]
⁺ ⁻
• pH = 7.0
•Acidic Solutions:
• [H ] > [OH ]
⁺ ⁻
• pH < 7.0
•Basic Solutions:
• [H ] < [OH ]
⁺ ⁻
• pH > 7.0
6.
6
Water itself isneutral, neither acidic
nor basic.
The pH of pure water is 7
A pH of 7 is termed neutral because [H+] and [OH−]
are equal
7.
7
Acid and base
An acid is a substance that can release hydrogen
ions(protons)
A base is a substance that can accept hydrogen
ions.
When dissolved in water, almost all the molecules
of a strong acid dissociate and release their
hydrogen ions
but only a small percentage of the total molecules
of a weak acid dissociate.
8.
8
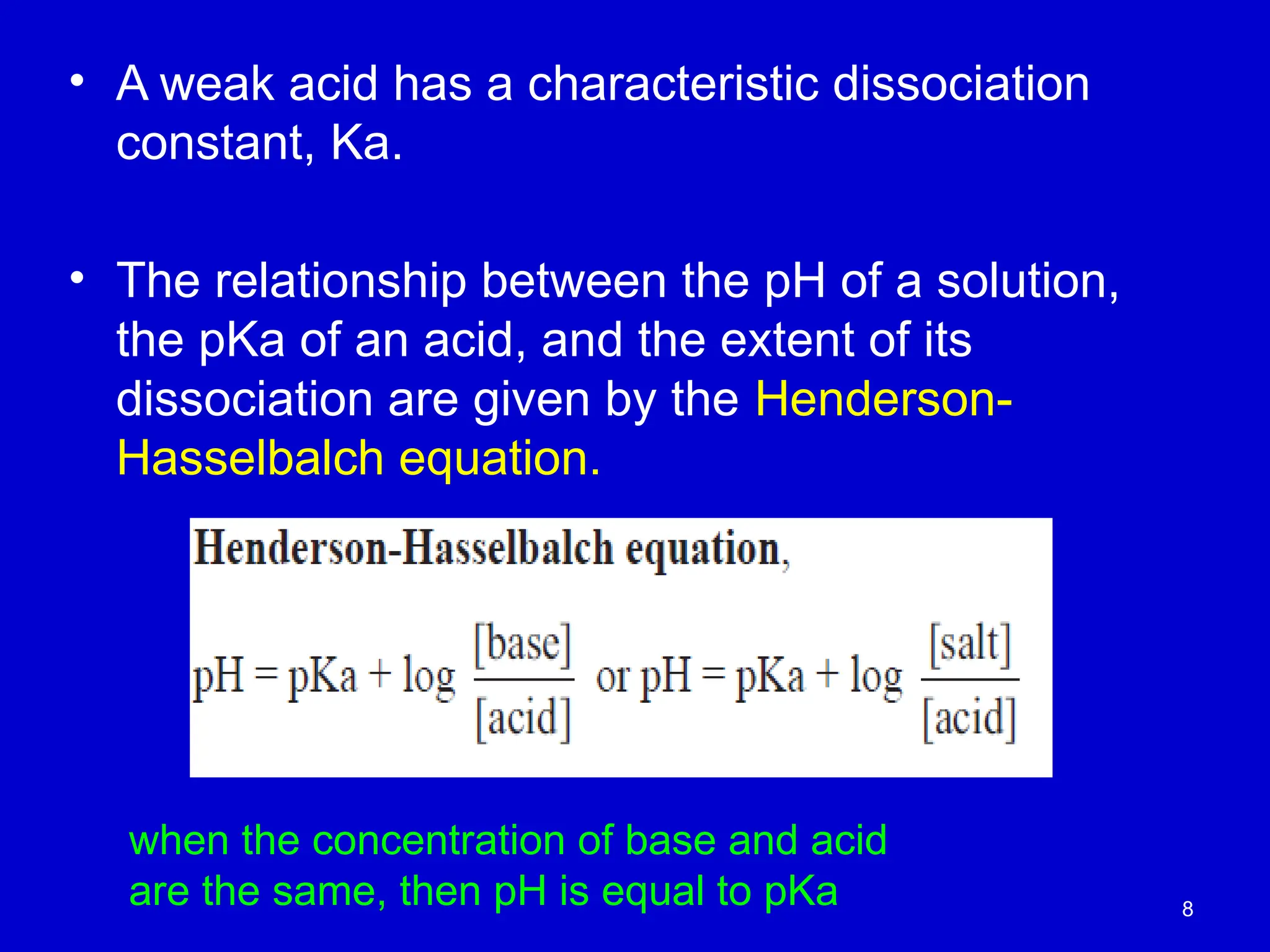
• A weakacid has a characteristic dissociation
constant, Ka.
• The relationship between the pH of a solution,
the pKa of an acid, and the extent of its
dissociation are given by the Henderson-
Hasselbalch equation.
when the concentration of base and acid
are the same, then pH is equal to pKa
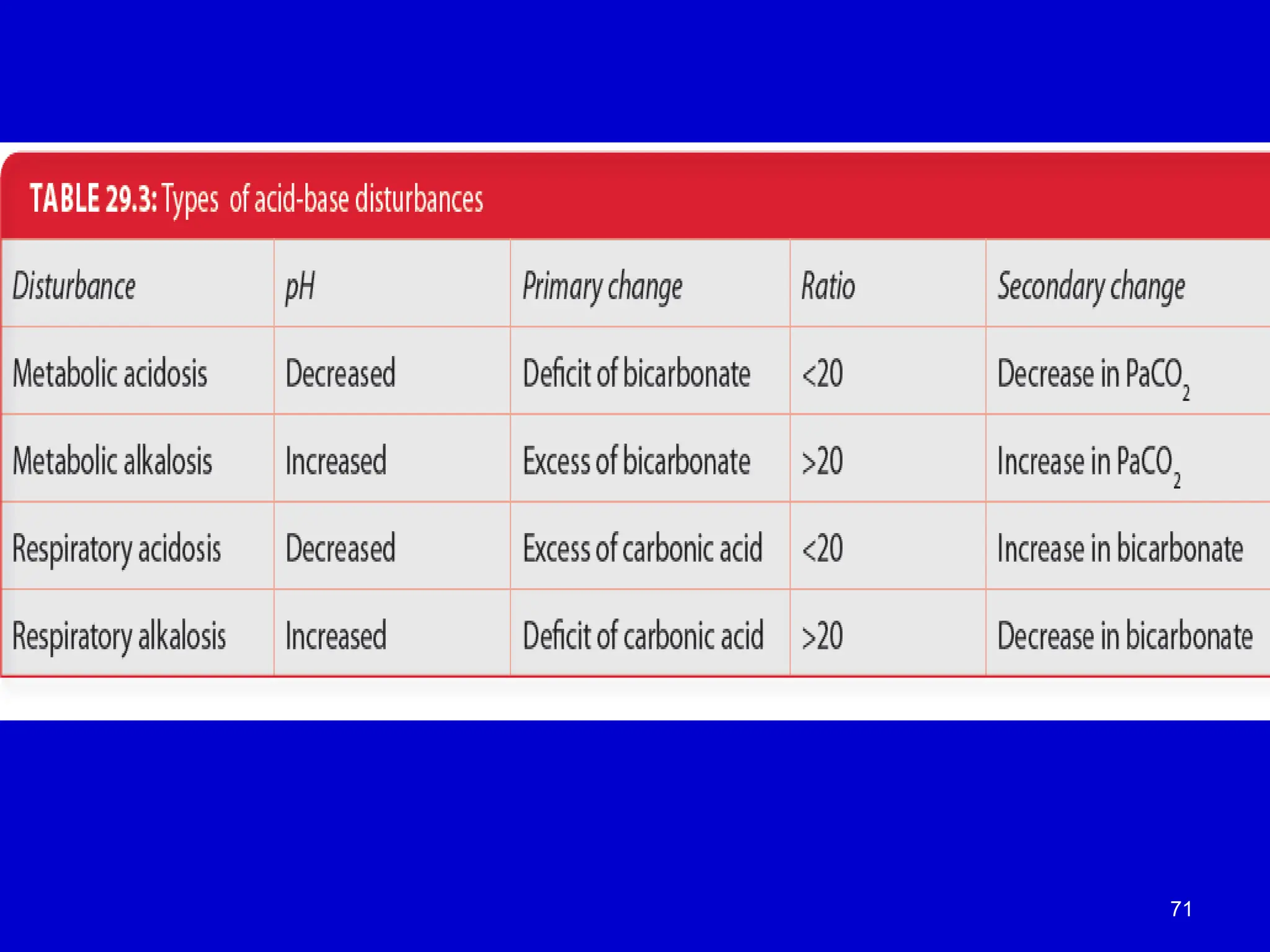
Acid-Base Disorders
• Acidosis
–[H+
] above normal (low pH)
– ratio [HCO3
-
/Pco2] < 20
• Alkalosis
– [H+
] below normal (high pH)
– ratio [HCO3
-
/Pco2] > 20
pH = pK + log[HCO3
-
/Pco2]
10
[HCO3 –
] = 24.0 mM, and [CO2]= 1.20 mM.
Normal values for these are pH = 7.40,
12.
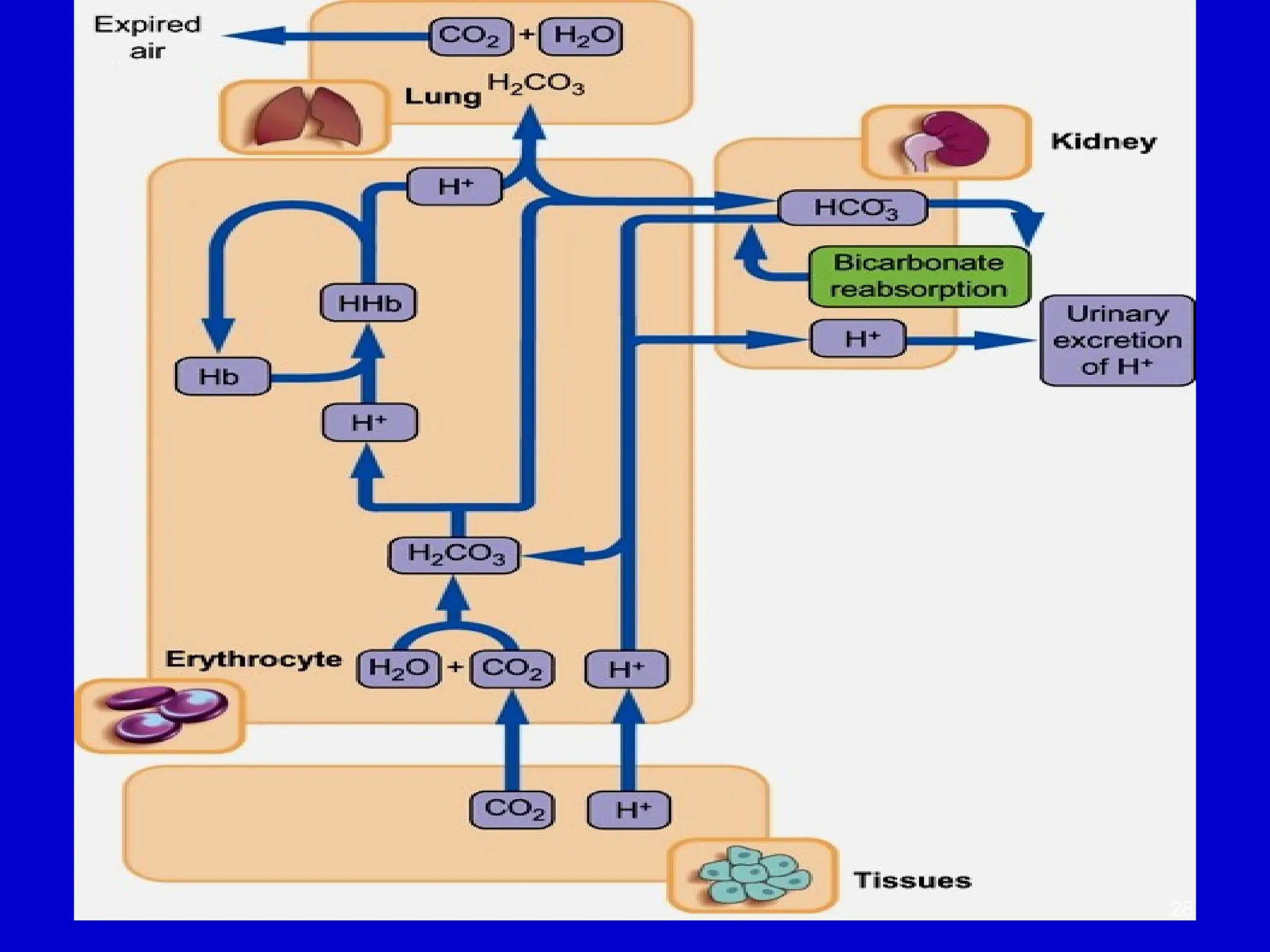
Maintaining the Acid-BaseBalance
• Key Players:
• Lungs: Regulate the exchange of CO and O between the
₂ ₂
blood and atmosphere.
• Erythrocytes (Red Blood Cells): Transport gases (O and
₂
CO ) between the lungs and tissues.
₂
• Kidneys: Control plasma bicarbonate synthesis and excrete
hydrogen ions (H ).
⁺
• Acid-Base Balance in Clinical Medicine:
• Essential for homeostasis.
• Crucial in specialties like Critical Care Medicine, Anesthesia,
Nephrology, and Respiratory Medicine.
• Clinical Relevance:
• Imbalances can lead to conditions like acidosis or alkalosis.
• Proper management is critical for patient outcomes in
emergency care and surgical settings.
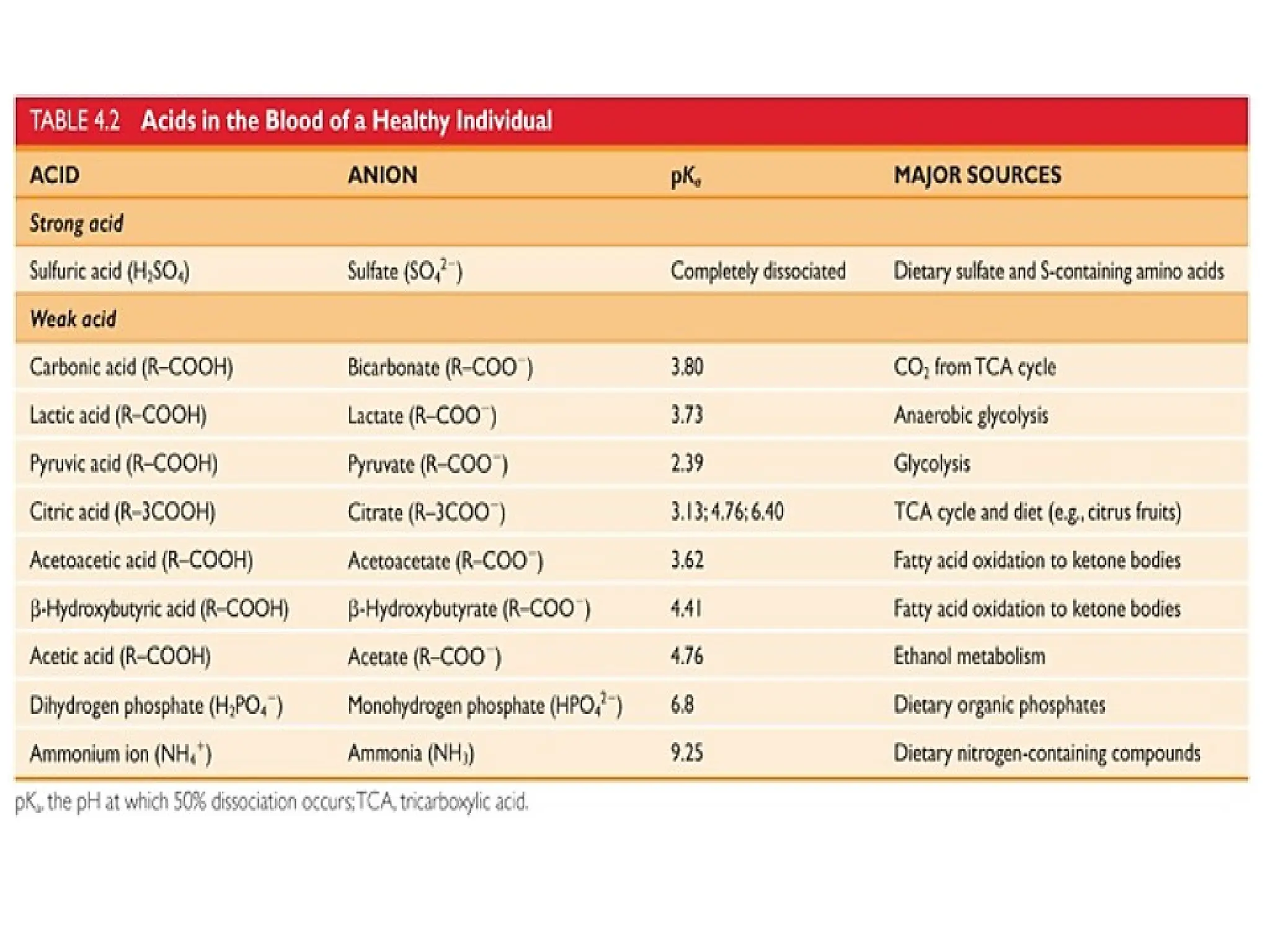
Acid Production fromNormal Fuel Metabolism
• Major Acids Produced:
• Carbonic Acid (H CO )
₂ ₃ :
• Formed from CO₂ and water, produced during the TCA
cycle and other oxidative pathways.
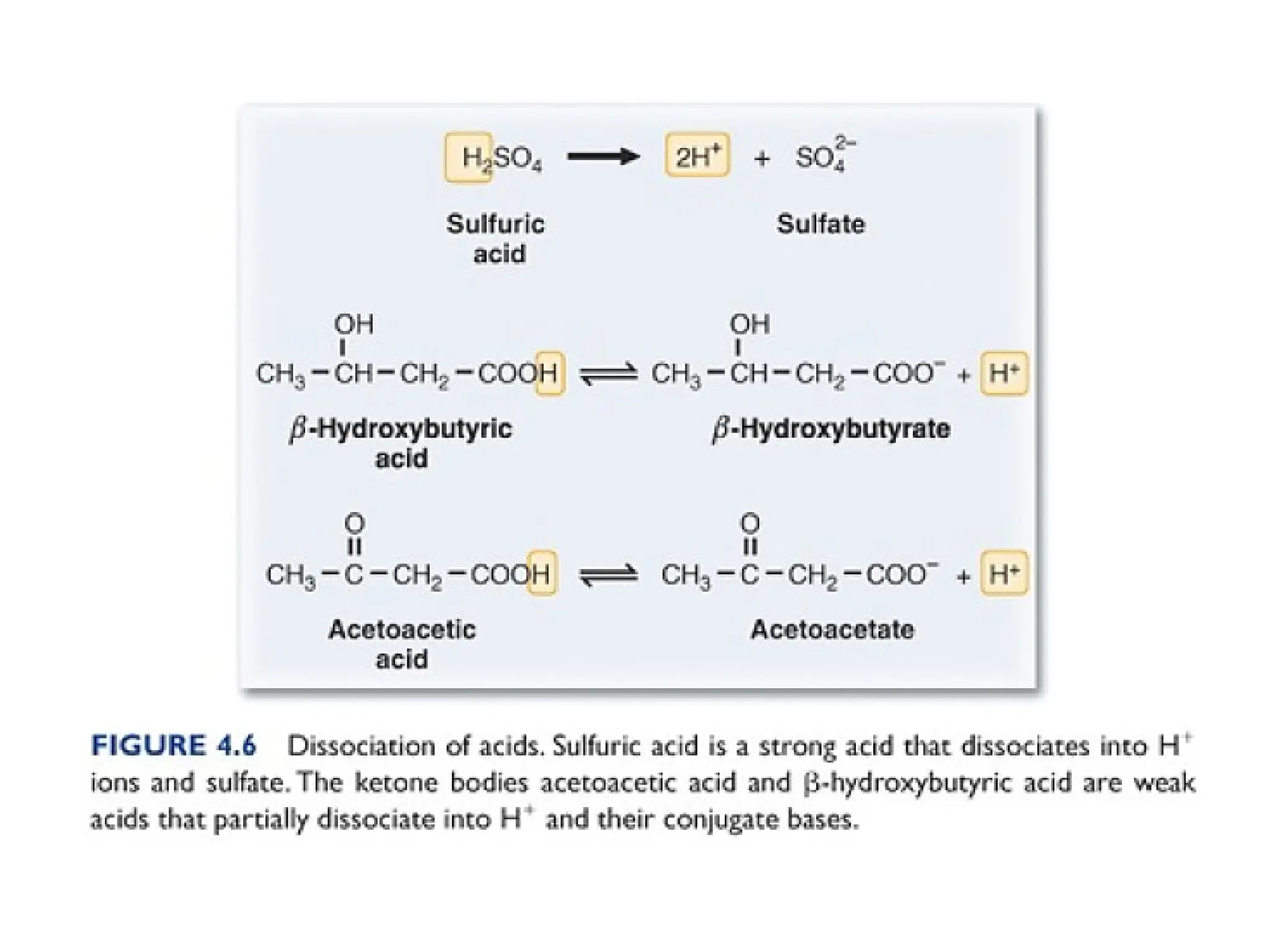
• Sulfuric Acid (H SO )
₂ ₄ :
• Produced from the oxidation of sulfur-containing amino
acids, methionine and cysteine.
• Sulfuric acid dissociates into H⁺ and SO ²
₄ ⁻, and both are
excreted.
• Phosphoric Acid:
• Produced by the hydrolysis of phosphate esters,
resulting in the equivalent of phosphoric acid.
• Daily Acid Production:
• On average, about 3 g of phosphoric acid and 3 g of
sulfuric acid are produced per day.
15.
Nonvolatile Acids inMetabolism
• Nonvolatile Acids:
• These acids are derived from sources other than CO₂.
• Cannot be removed by the lungs, unlike volatile acids like CO .
₂
• Must be excreted via the kidneys.
• Types of Nonvolatile Acids:
• Lactic Acid:
• Produced during anaerobic metabolism (hypoxia).
• Accumulation is a hallmark of conditions like hypoxia or shock.
• Ketoacids (Acetoacetate and β-hydroxybutyrate):
• Produced during ketogenesis, often in conditions like diabetes.
• Excess ketoacids can lead to ketoacidosis in diabetic patients.
• Daily Production:
• The net production of nonvolatile acids is approximately 50 mmol/24 hours.
• Clinical Relevance:
• Monitoring and managing the excretion of nonvolatile acids is crucial in
conditions like diabetic ketoacidosis and lactic acidosis.
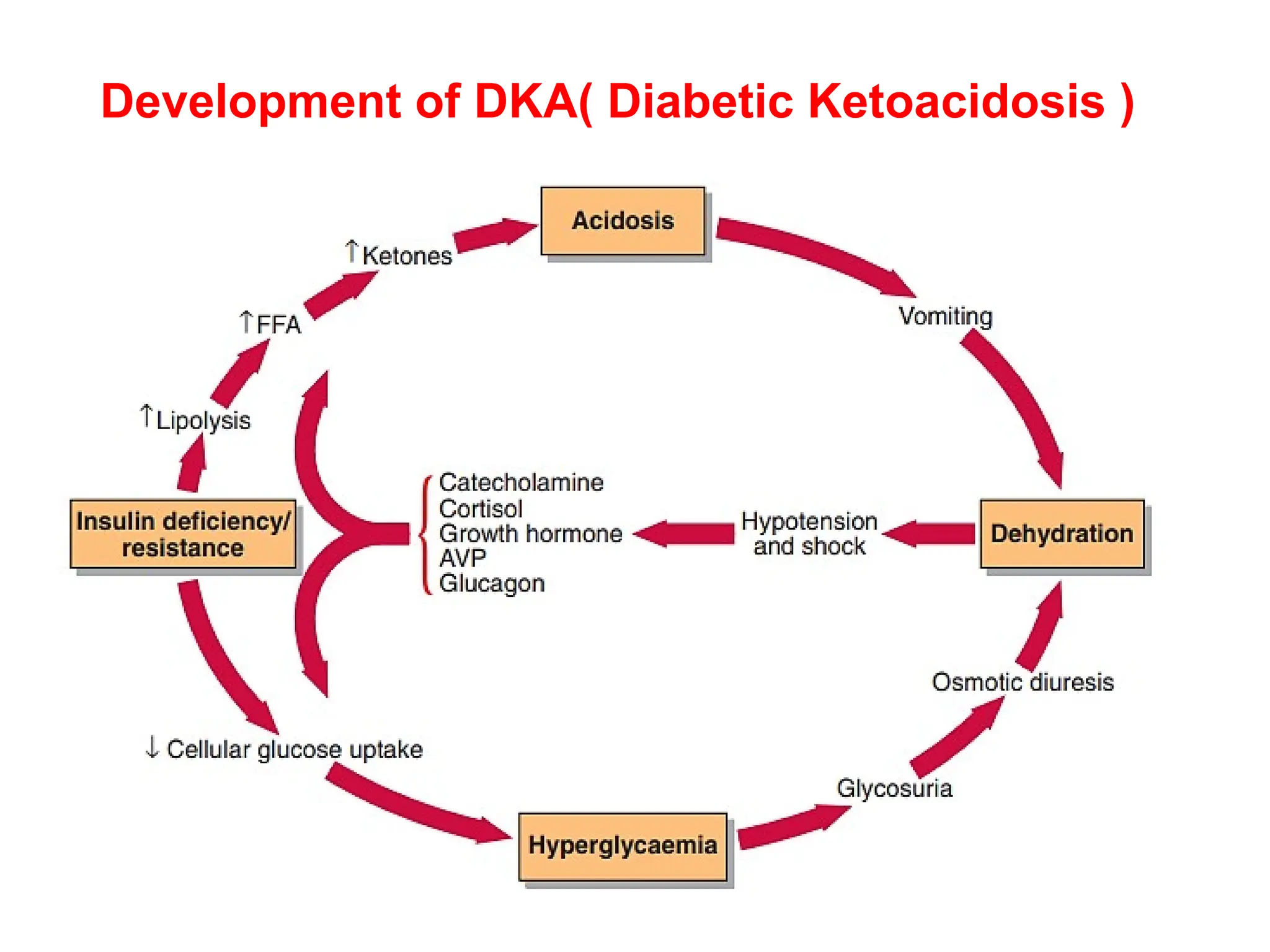
Diabetic Ketoacidosis (DKA)and Insulin Deficiency
in Type 1 Diabetes Mellitus (T1DM)
• Insulin Deficiency and Fat Metabolism:
• In Type 1 Diabetes Mellitus (T1DM), low insulin levels lead to:
• Release of free fatty acids (FFAs) from adipocytes (fat cells).
• The liver converts FFAs into ketone bodies (KBs), including acetoacetate and
β-hydroxybutyrate.
• Ketone Bodies and Acidosis:
• Ketone bodies are weak acids that dissociate into:
• Acetoacetate and β-hydroxybutyrate (anions) and hydrogen ions (H )
⁺ .
• This leads to a decrease in blood pH, causing metabolic acidosis.
• Development of Diabetic Ketoacidosis (DKA):
• As ketone bodies accumulate in the blood, they cause a significant drop in pH, leading
to DKA.
• DKA is characterized by:
• High blood glucose.
• Elevated ketone levels in the blood and urine.
• Metabolic acidosis.
20.
Buffers and pHRegulation
• Definition of a Buffer:
• Composed of a weak acid and its conjugate base.
• Helps resist changes in pH when H⁺ (hydrogen ions) or
OH⁻ (hydroxide ions) are added.
• Buffer Capacity:
• A buffer can compensate for pH changes within
approximately 1 pH unit of its pKa.
• Effective Range:
• The effective buffering range is 1 pH unit above or
below the pKa.
• Importance in Biological Systems:
• Buffers are essential in maintaining acid-base balance
in blood and other bodily fluids.
21.
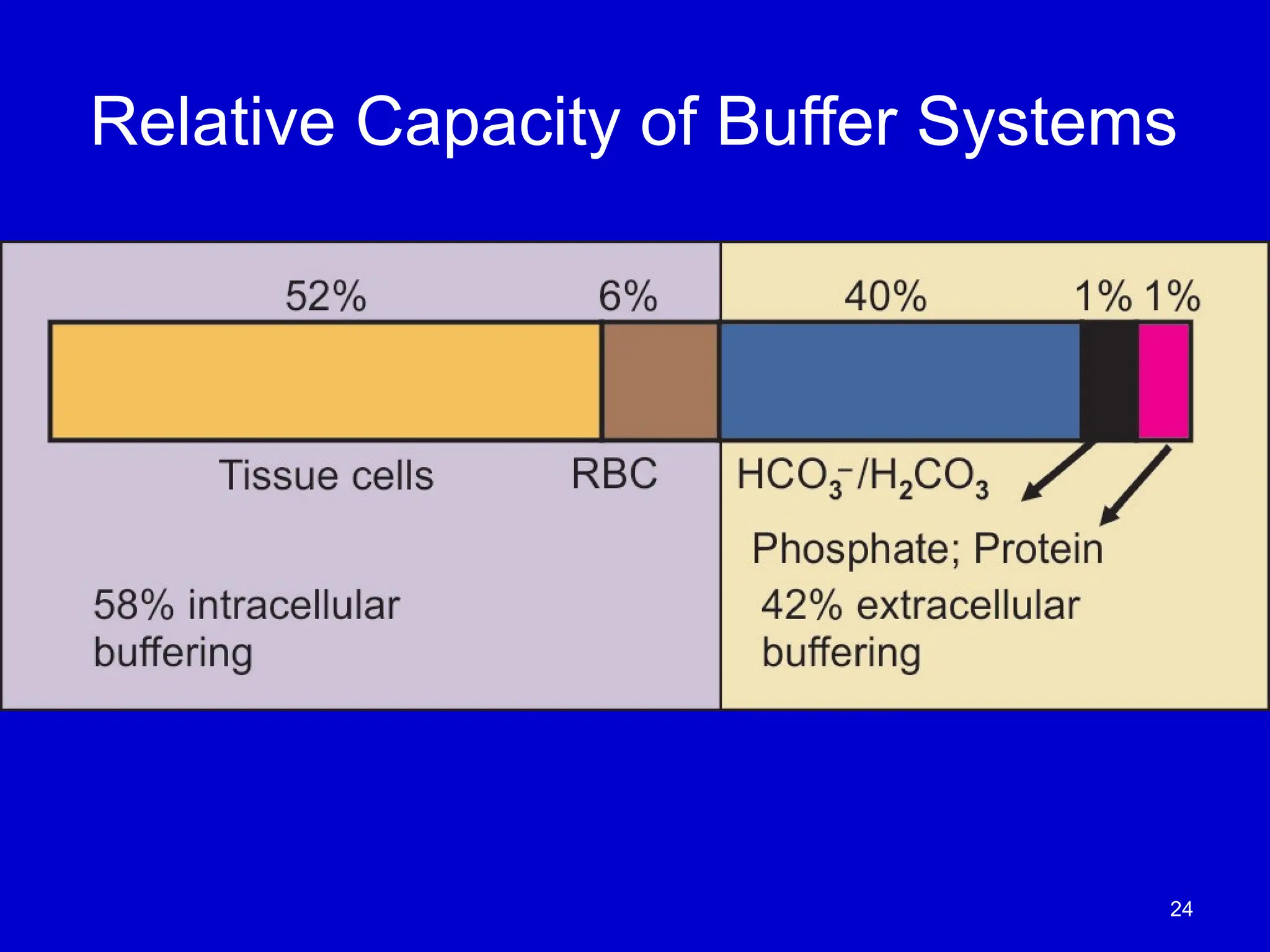
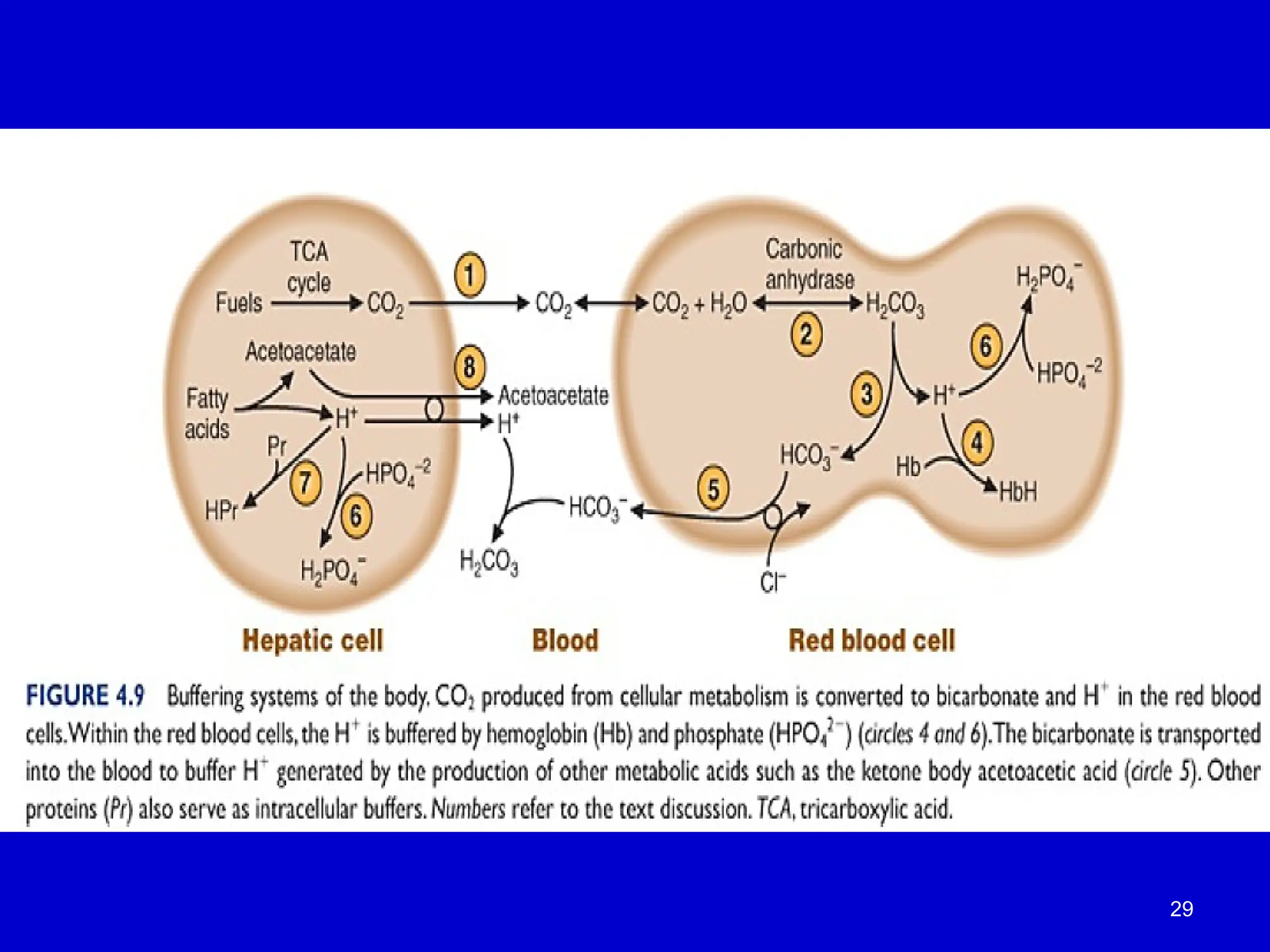
Buffer Systems inBlood and Tissues
• Bicarbonate Buffer:
• The primary buffer in blood that neutralizes hydrogen ions (H )
⁺ released from
cells.
• Works through the carbonic acid (H CO )
₂ ₃ and bicarbonate (HCO )
₃⁻ equilibrium.
• Hemoglobin as a Buffer:
• Hemoglobin buffers hydrogen ions generated from the carbonic anhydrase
reaction in red blood cells.
• Important in buffering CO₂ transport and maintaining blood pH.
• Intracellular Buffers:
• In cells, buffering is mainly carried out by:
• Proteins: Act as amphoteric buffers (both acid and base properties).
• Phosphates: Contribute to buffering by neutralizing H⁺ ions.
• Overall Importance:
• Buffer systems work to minimize changes in hydrogen ion concentration and
maintain pH homeostasis in both blood and tissues.
22.
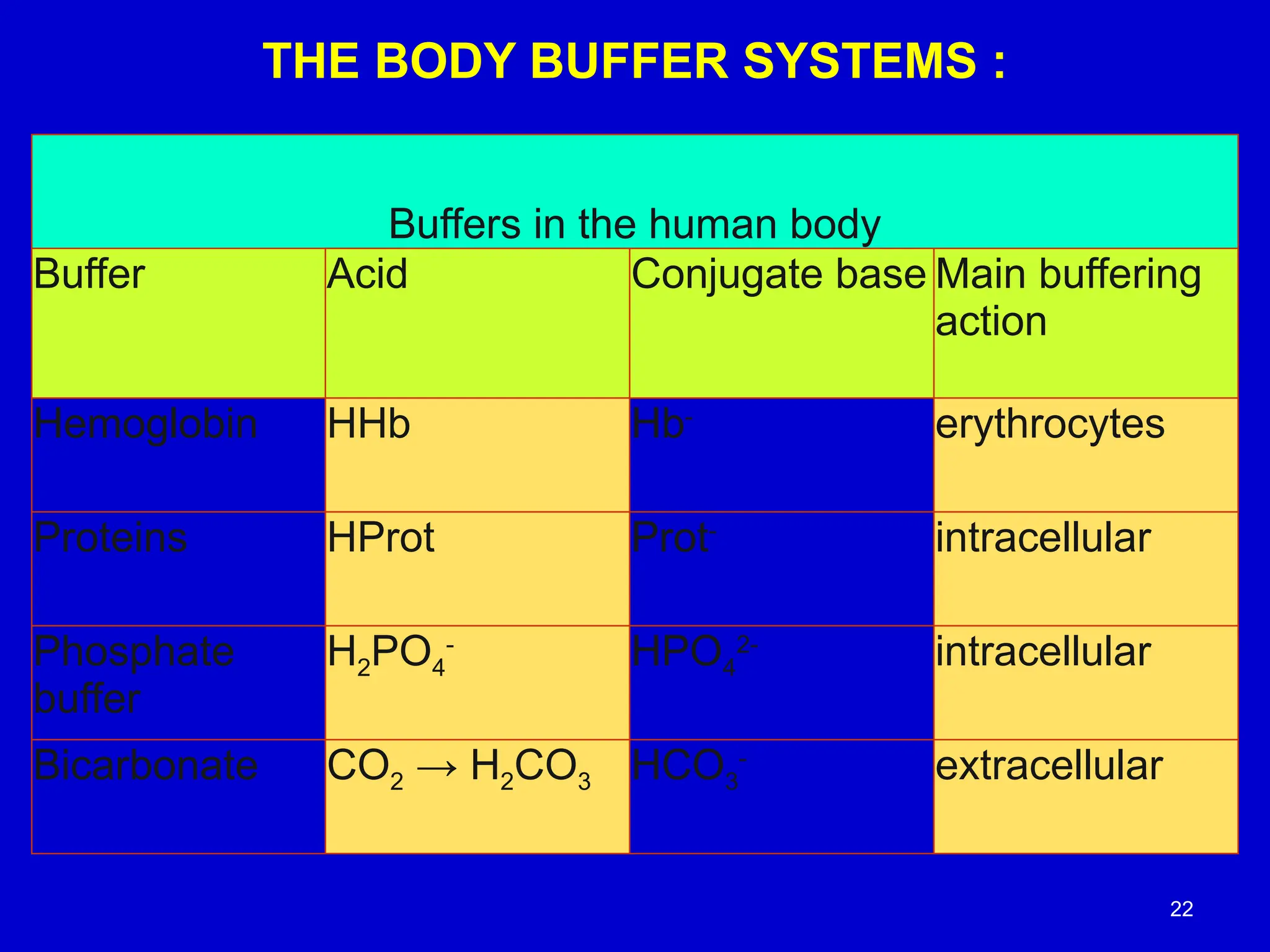
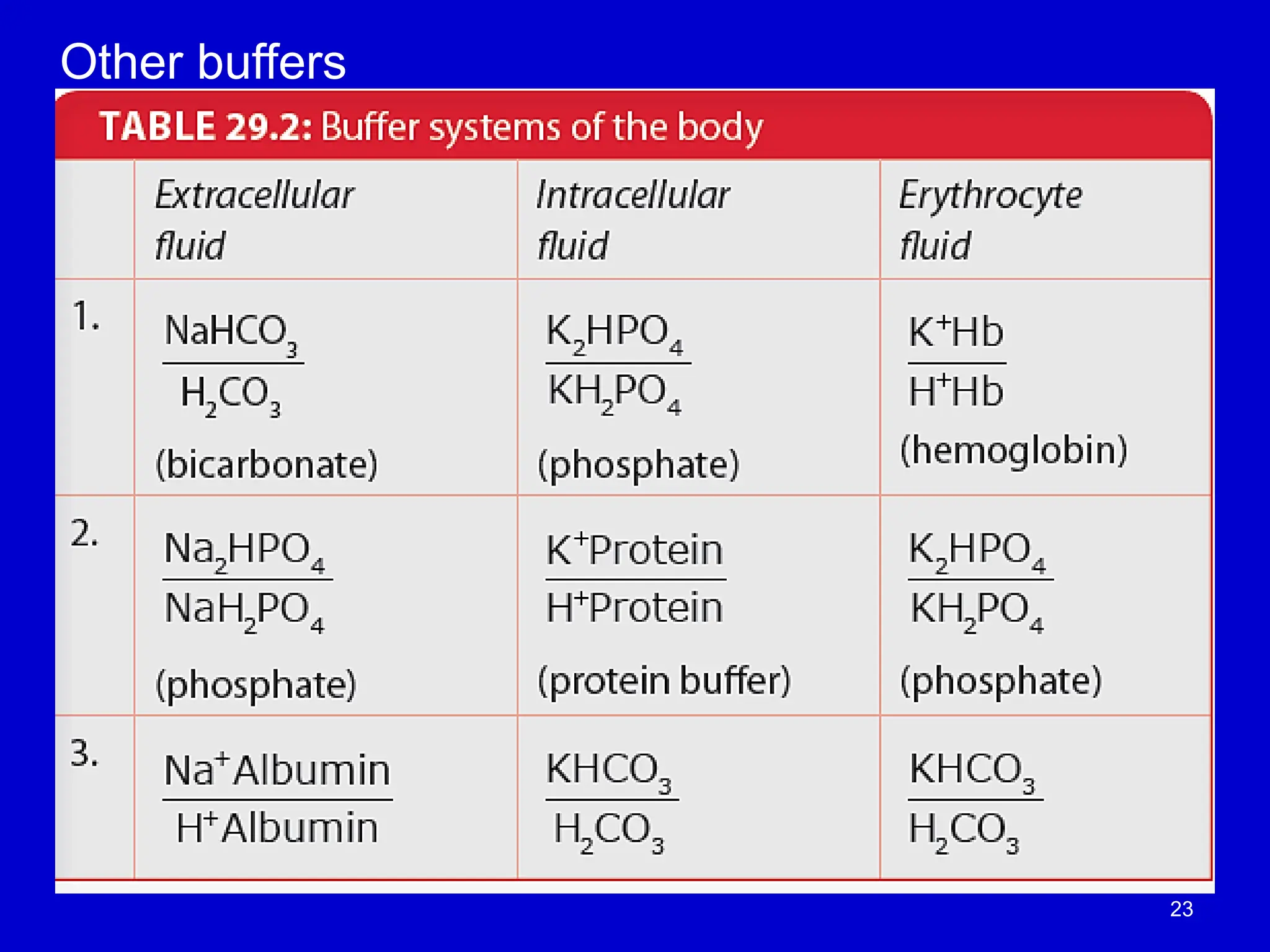
THE BODY BUFFERSYSTEMS :
Buffers in the human body
Buffer Acid Conjugate base Main buffering
action
Hemoglobin HHb Hb-
erythrocytes
Proteins HProt Prot-
intracellular
Phosphate
buffer
H2PO4
-
HPO4
2-
intracellular
Bicarbonate CO2 → H2CO3 HCO3
-
extracellular
22
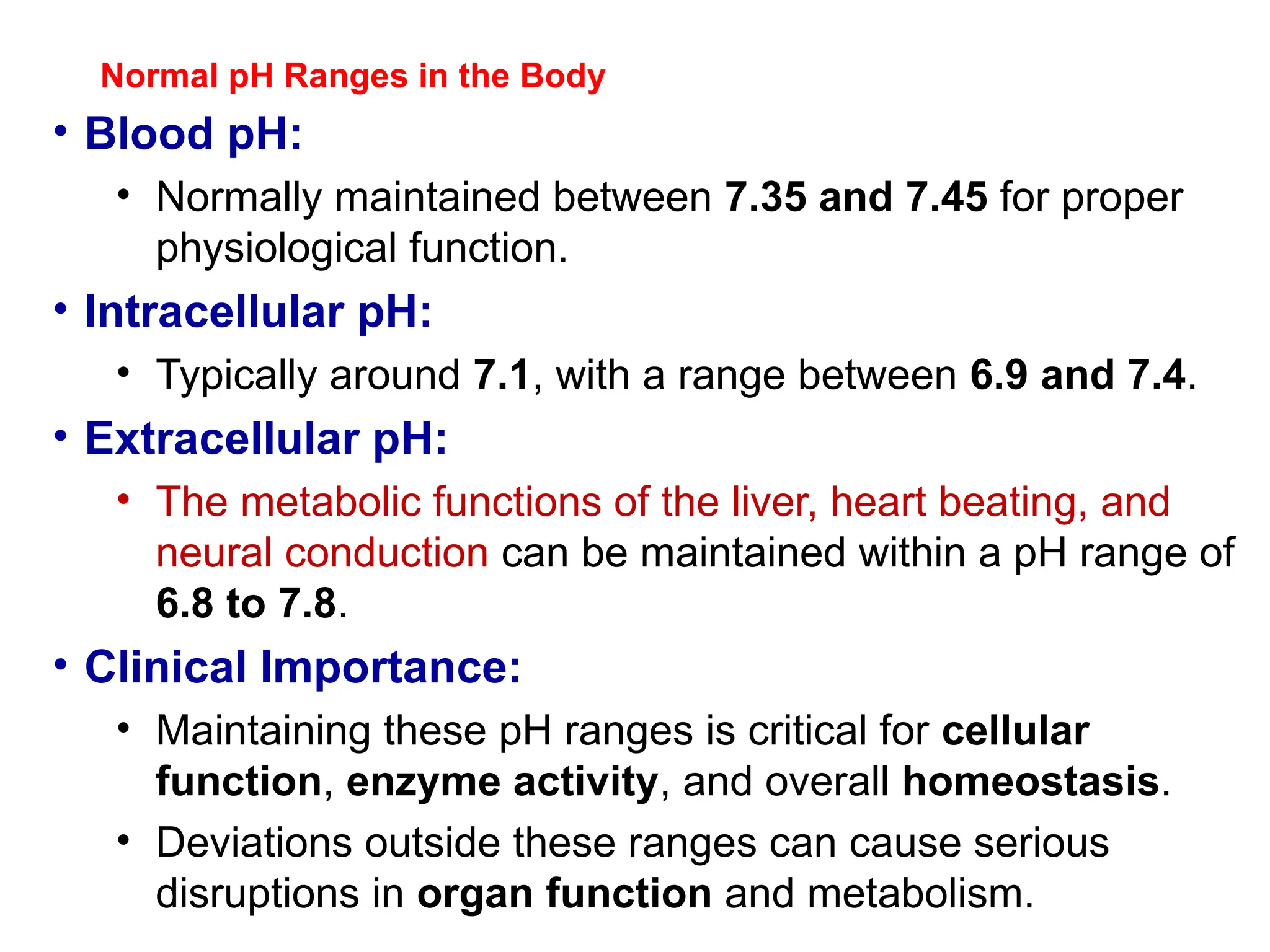
Normal pH Rangesin the Body
• Blood pH:
• Normally maintained between 7.35 and 7.45 for proper
physiological function.
• Intracellular pH:
• Typically around 7.1, with a range between 6.9 and 7.4.
• Extracellular pH:
• The metabolic functions of the liver, heart beating, and
neural conduction can be maintained within a pH range of
6.8 to 7.8.
• Clinical Importance:
• Maintaining these pH ranges is critical for cellular
function, enzyme activity, and overall homeostasis.
• Deviations outside these ranges can cause serious
disruptions in organ function and metabolism.
27.
Bicarbonate-Carbonic Acid BufferSystem
• Importance of the Buffer System:
• The bicarbonate-carbonic acid buffer is the most important
buffer system in the body.
• Key Reasons:
• High Concentrations of Bicarbonate:
• Bicarbonate (HCO ) is present in relatively
₃⁻ high
concentrations in the blood, making it an effective buffer.
• Physiological Control:
• The components of this system are tightly regulated by
the body:
• CO₂ levels are controlled by the lungs through ventilation.
• Bicarbonate (HCO )
₃⁻ levels are controlled by the kidneys
through reabsorption and excretion.
.
Hemoglobin as aBuffer (His-buffer)
• Hemoglobin and pH Regulation:
• Hemoglobin (Hb) helps buffer hydrogen ions (H ) released during the
⁺
dissociation of carbonic acid (H CO )
₂ ₃ in red blood cells.
• Role of Histidine:
• The histidine side chain in hemoglobin has a pKa of 6.7, allowing it to
effectively accept protons (H )
⁺ .
• This histidine residue acts as a buffer, helping to neutralize H and maintain
⁺
pH balance.
• Mechanism:
• As carbonic acid dissociates into H⁺ and HCO₃⁻, the H ions are
⁺ buffered
by hemoglobin's histidine residues.
• This plays a crucial role in CO transport
₂ and pH regulation in the blood.
• Clinical Relevance:
• Hemoglobin's buffering capacity helps maintain the acid-base balance during
respiratory gas exchange and prevents significant pH changes.
31.
Extracellular Proteins andTheir Role in Buffering
• Extracellular Proteins:
• Albumin and other extracellular proteins play a key role in
maintaining the blood's buffering capacity.
• Mechanism:
• These proteins contain amino acid side chains that can accept and
release protons (H )
⁺ .
• The ability of these amino acid residues (like histidine) to bind and
release protons helps neutralize excess H⁺ and maintain blood pH.
• Clinical Relevance:
• The buffering capacity of extracellular proteins is essential for
maintaining acid-base balance in the blood, particularly in regulating
pH during metabolic processes.
• Importance of Albumin:
• Albumin is the most abundant extracellular protein in blood, making
it a critical player in extracellular buffering.
32.
Phosphate Buffer System
•Role in Buffering:
• Phosphate anions play a major role as an intracellular buffer.
• Red blood cells and other cell types have much higher
concentrations of phosphate compared to blood and interstitial
fluid.
• Mechanism:
• Phosphate buffers work similarly to the bicarbonate buffer
system, where phosphate ions can accept or donate protons
(H ) to help maintain pH stability.
⁺
• Organic Phosphate Buffers:
• Organic phosphate anions such as glucose-6-phosphate and
ATP also act as important buffers inside cells.
• Clinical Relevance:
• The phosphate buffer system is crucial for maintaining pH
stability within cells, especially during metabolic processes,
where H⁺ production can fluctuate.
33.
33
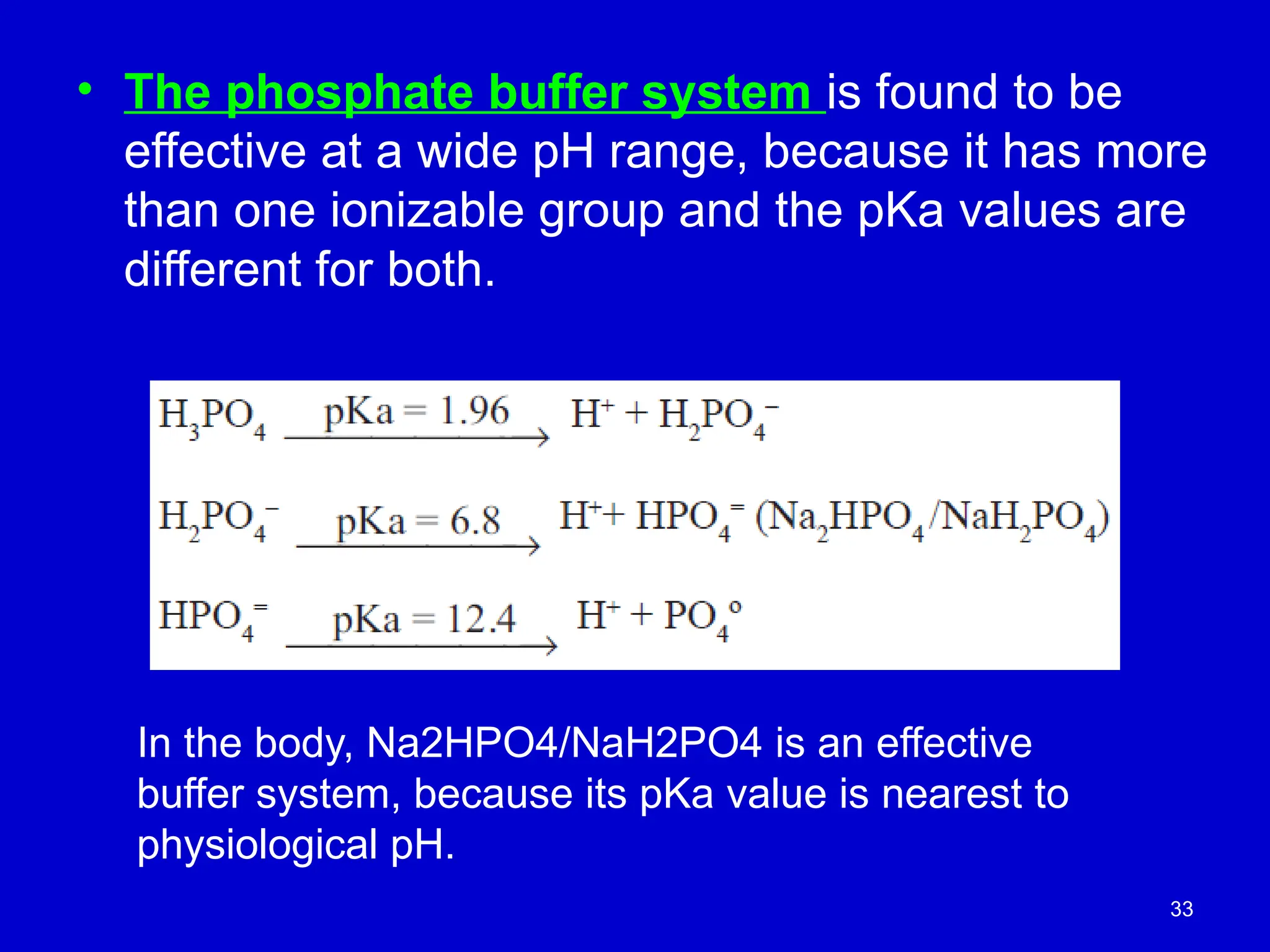
• The phosphatebuffer system is found to be
effective at a wide pH range, because it has more
than one ionizable group and the pKa values are
different for both.
In the body, Na2HPO4/NaH2PO4 is an effective
buffer system, because its pKa value is nearest to
physiological pH.
34.
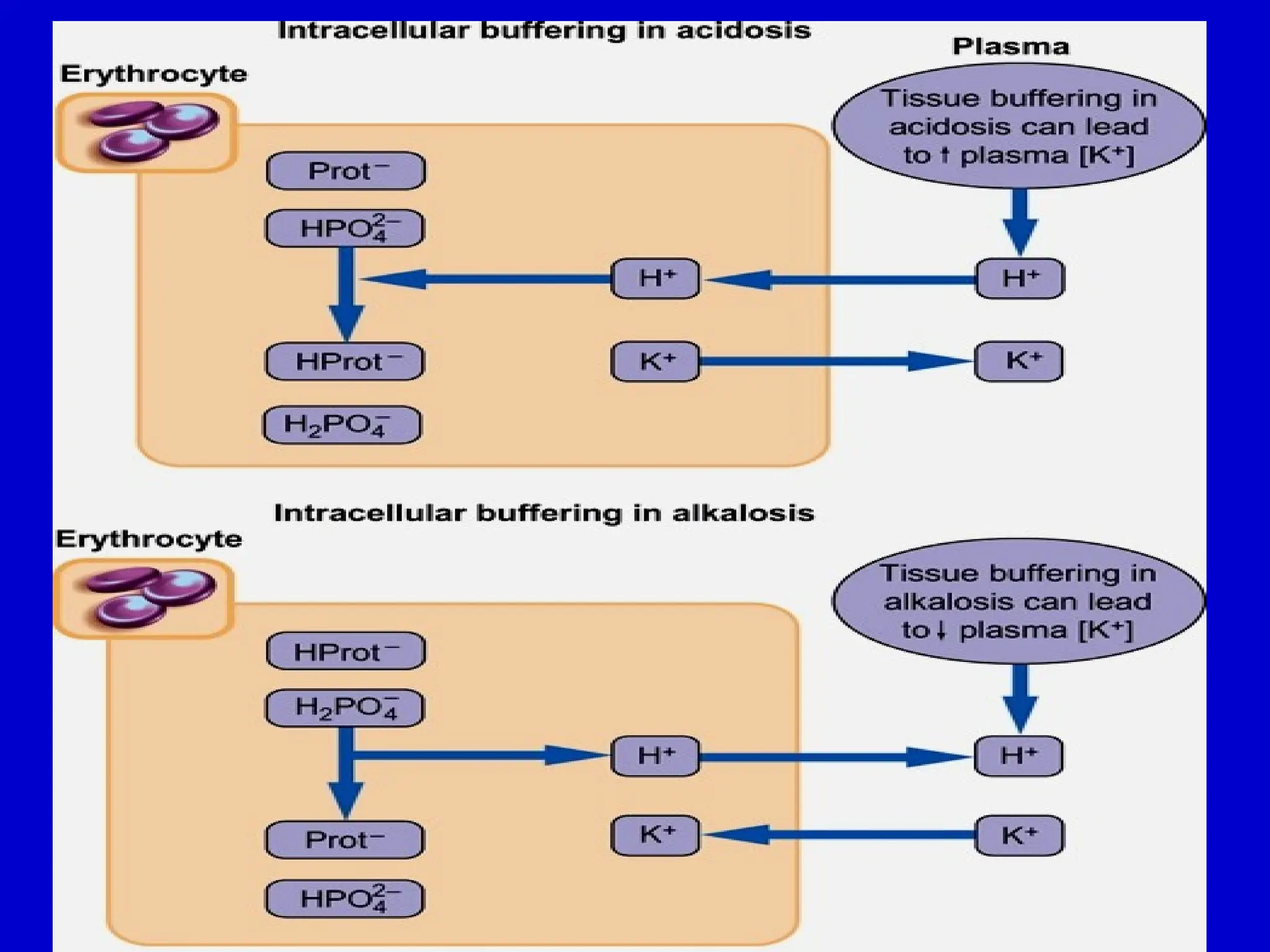
Intracellular Buffering andPotassium Exchange
• Intracellular Buffers:
• Proteins (e.g., hemoglobin, albumin) and phosphates are the
primary buffers inside cells.
• Mechanism of Buffering:
• Hydrogen ions (H )
⁺ enter cells in exchange for potassium
ions (K )
⁺ , which can result in a temporary increase in
plasma potassium concentration.
• Changes in Plasma pH:
• Decreased plasma H⁺ (alkalosis) or bicarbonate excess is
buffered by intracellular H⁺.
• As H⁺ exits the cell, it enters the plasma, and potassium moves
into the cell, leading to a decrease in plasma potassium levels.
• Clinical Relevance:
• This exchange between H and K helps maintain
⁺ ⁺ acid-base
balance, but can also affect plasma potassium levels,
especially in conditions like acidosis or alkalosis.
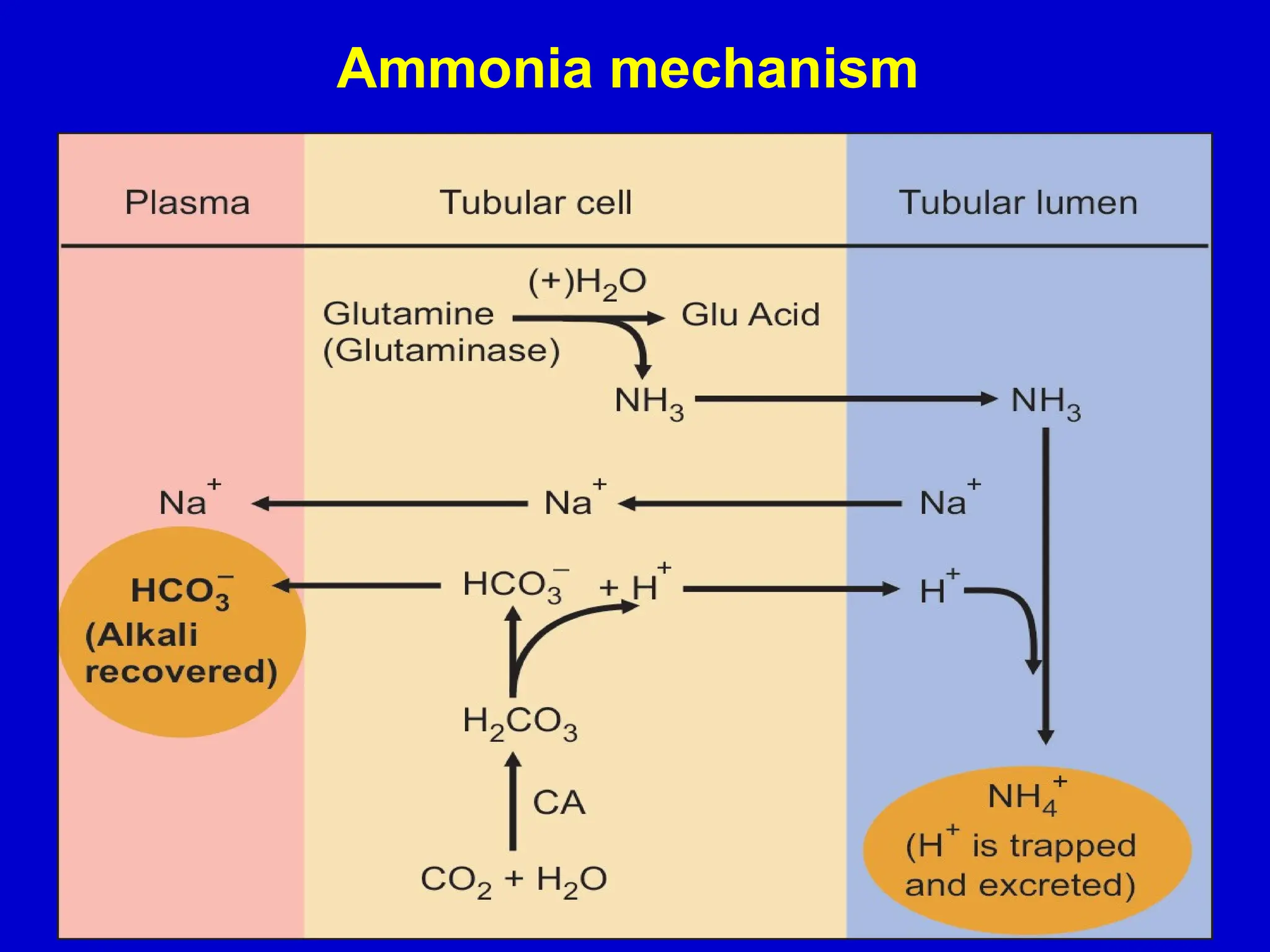
Renal Regulation ofpH
• Kidney Function in pH Regulation:
• The kidneys play a critical role in regulating the pH of extracellular fluid by
maintaining the balance between acids and bases.
• Urine pH:
• Normal urine pH is around 6, which is more acidic than extracellular fluid (pH = 7.4).
• Urine pH can vary from 4.5 to 9.8, depending on the amount of acid excreted by the
kidneys.
• Major Renal Mechanisms for pH Regulation:
• Excretion of H (Hydrogen ions)
⁺ :
• The kidneys excrete hydrogen ions to help lower body acidity.
• Reabsorption of Bicarbonate (HCO )
₃⁻ :
• Bicarbonate ions are reabsorbed in the kidneys to help maintain blood pH.
• Excretion of Titratable Acid (Net Acid Excretion):
• The kidneys excrete acids that can be titratable (e.g., phosphate), contributing to overall
acid removal.
• Excretion of NH (Ammonium ions)
₄⁺ :
• Ammonium ions are excreted, helping to neutralize acids and regulate pH.
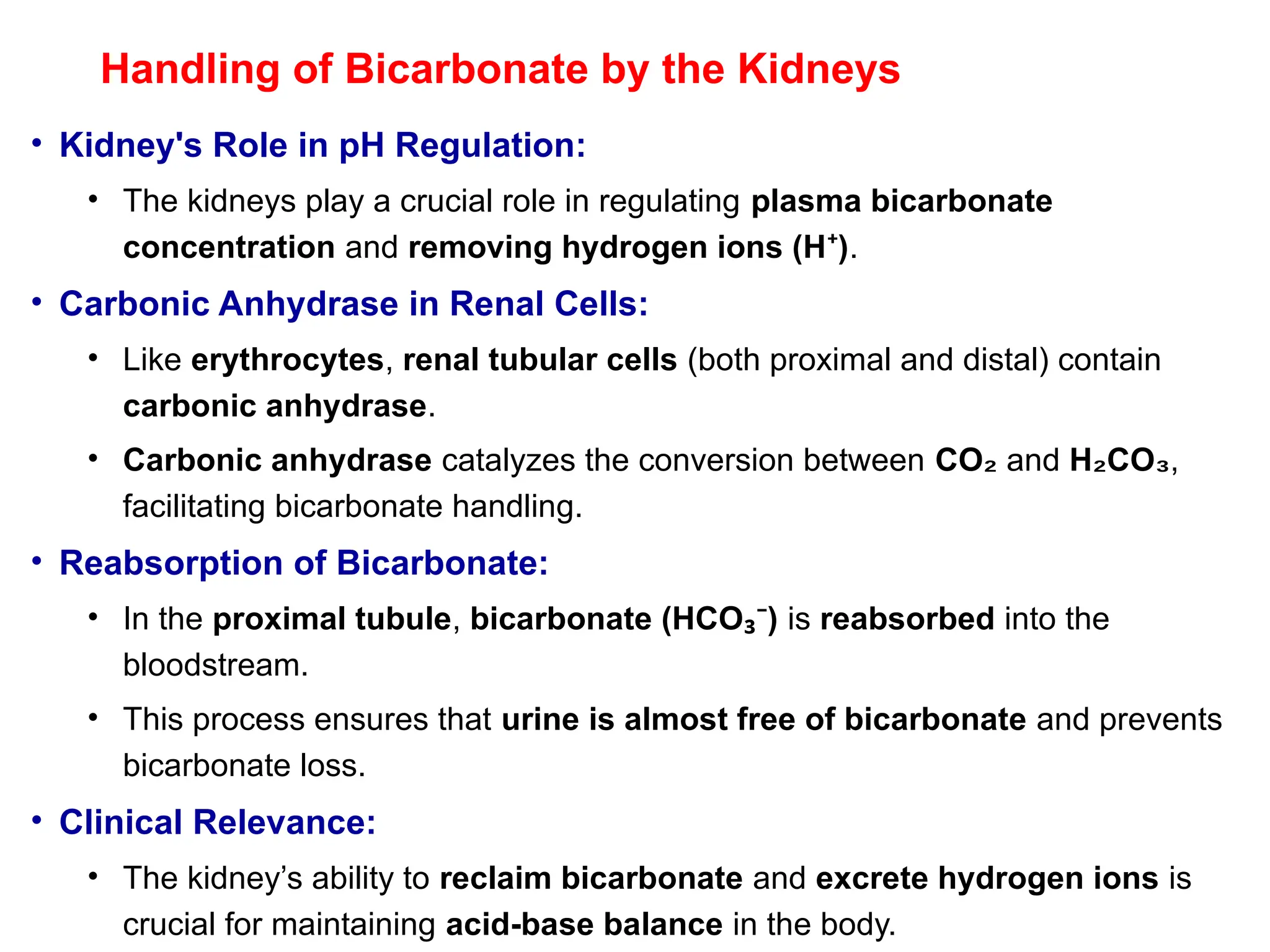
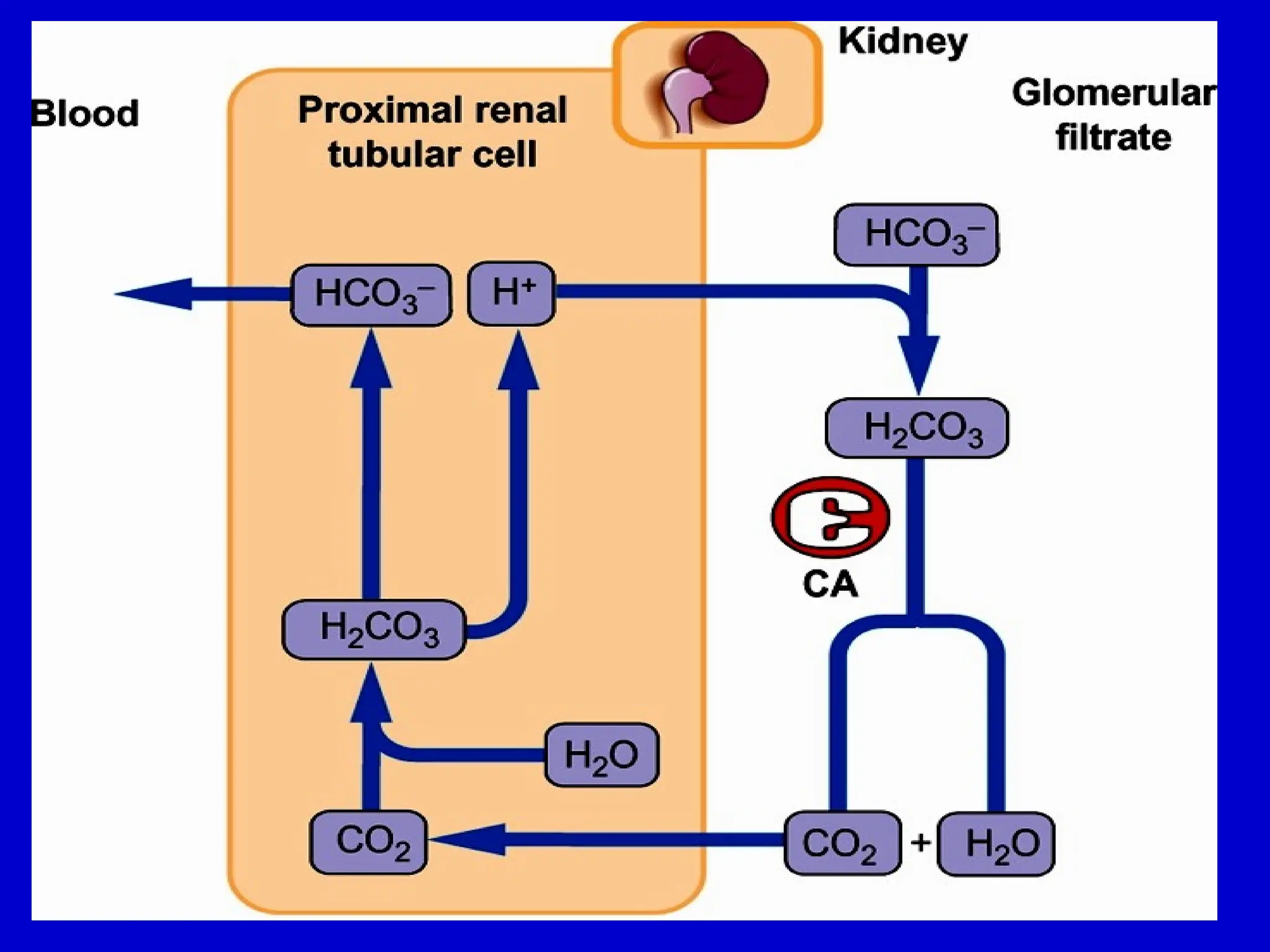
Handling of Bicarbonateby the Kidneys
• Kidney's Role in pH Regulation:
• The kidneys play a crucial role in regulating plasma bicarbonate
concentration and removing hydrogen ions (H )
⁺ .
• Carbonic Anhydrase in Renal Cells:
• Like erythrocytes, renal tubular cells (both proximal and distal) contain
carbonic anhydrase.
• Carbonic anhydrase catalyzes the conversion between CO₂ and H CO
₂ ₃,
facilitating bicarbonate handling.
• Reabsorption of Bicarbonate:
• In the proximal tubule, bicarbonate (HCO )
₃⁻ is reabsorbed into the
bloodstream.
• This process ensures that urine is almost free of bicarbonate and prevents
bicarbonate loss.
• Clinical Relevance:
• The kidney’s ability to reclaim bicarbonate and excrete hydrogen ions is
crucial for maintaining acid-base balance in the body.
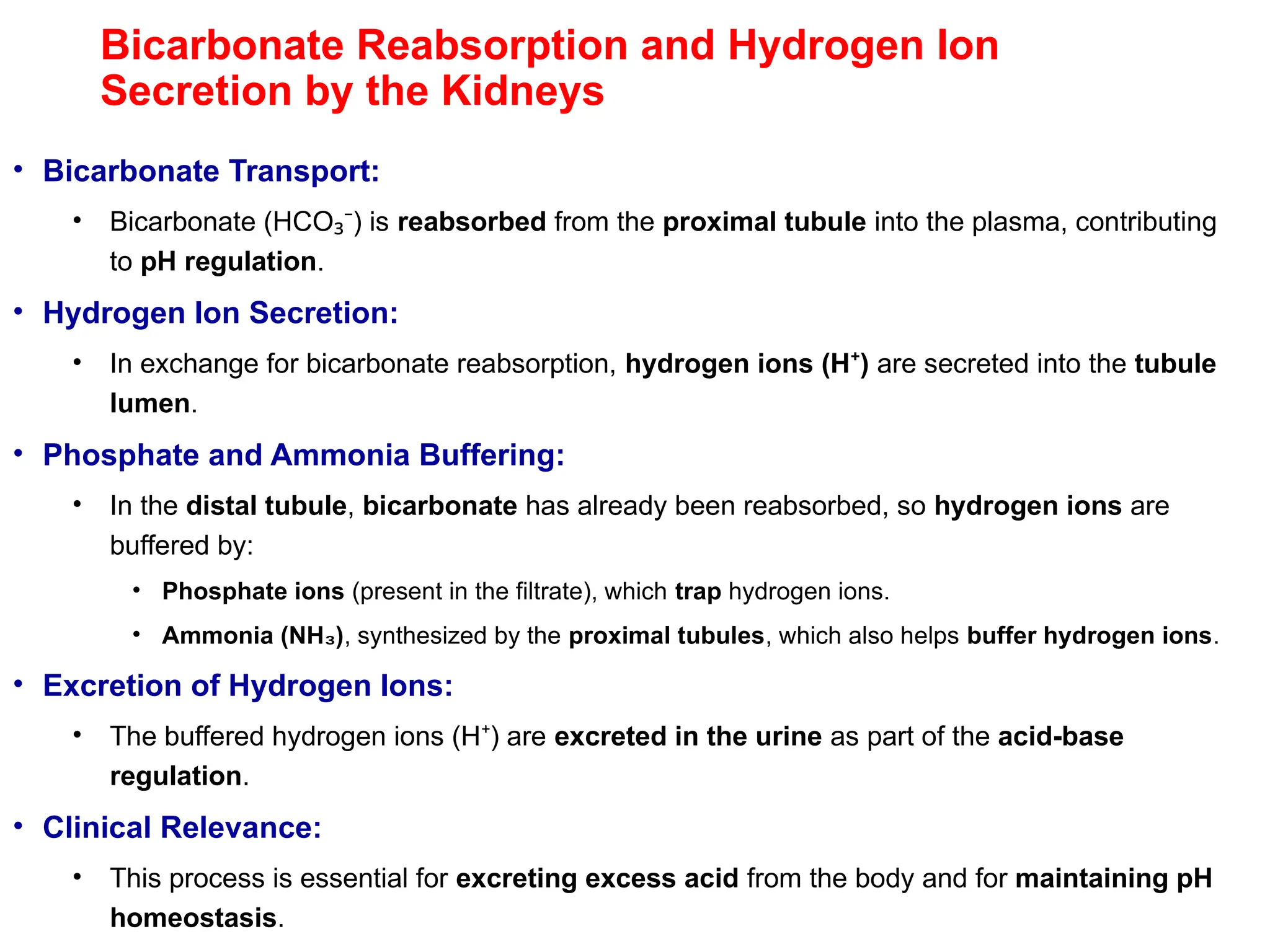
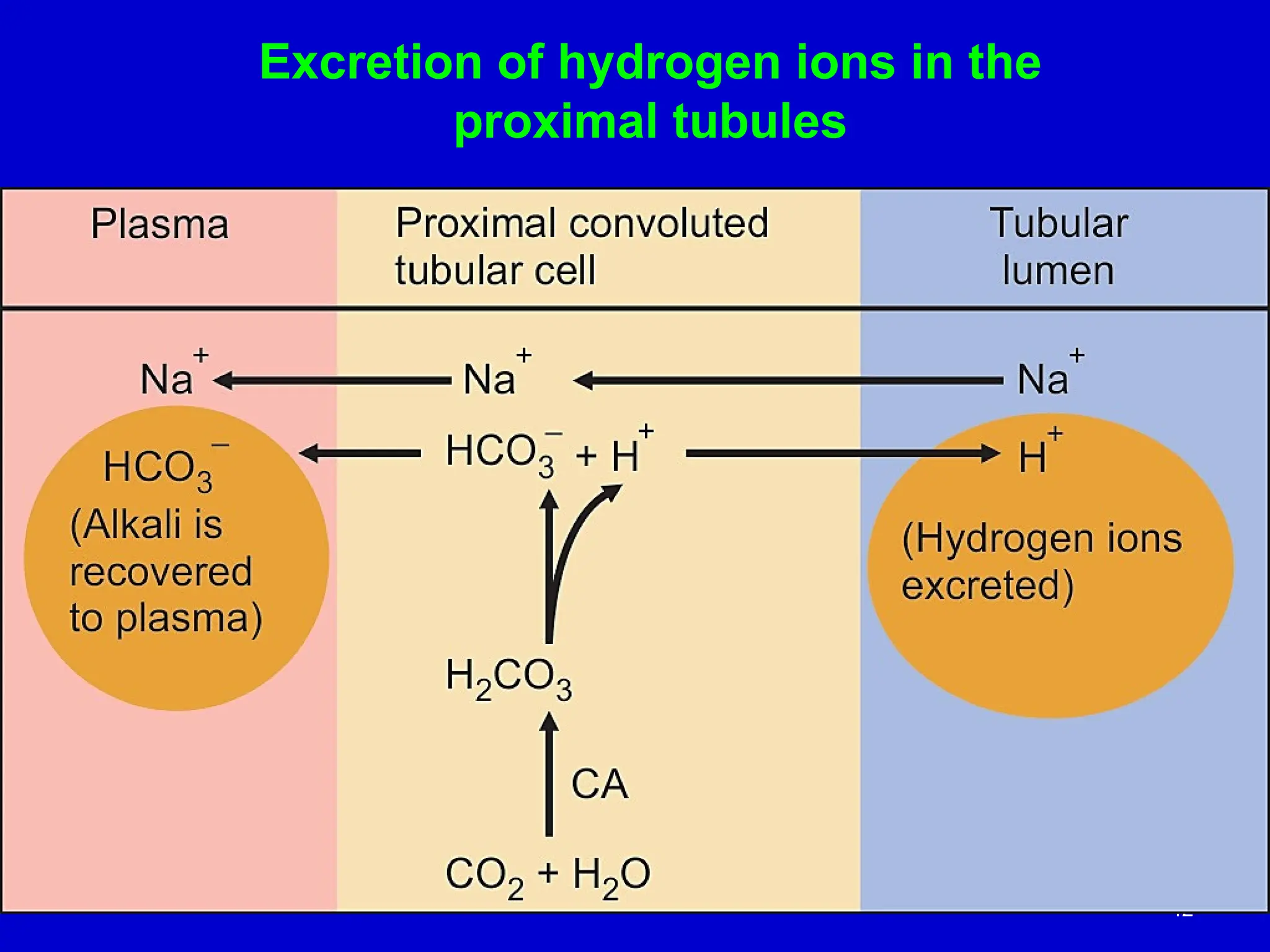
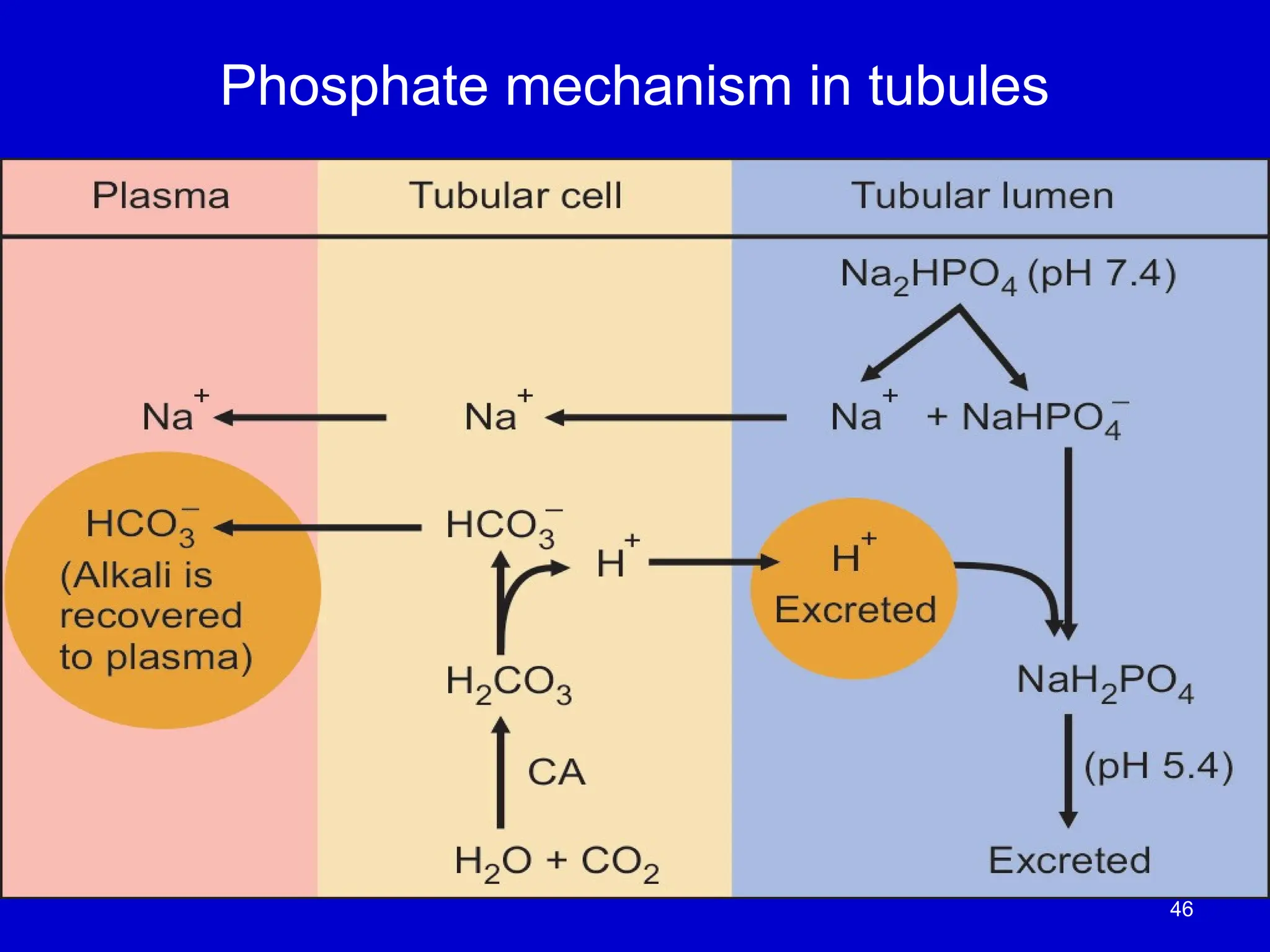
Bicarbonate Reabsorption andHydrogen Ion
Secretion by the Kidneys
• Bicarbonate Transport:
• Bicarbonate (HCO ) is
₃⁻ reabsorbed from the proximal tubule into the plasma, contributing
to pH regulation.
• Hydrogen Ion Secretion:
• In exchange for bicarbonate reabsorption, hydrogen ions (H )
⁺ are secreted into the tubule
lumen.
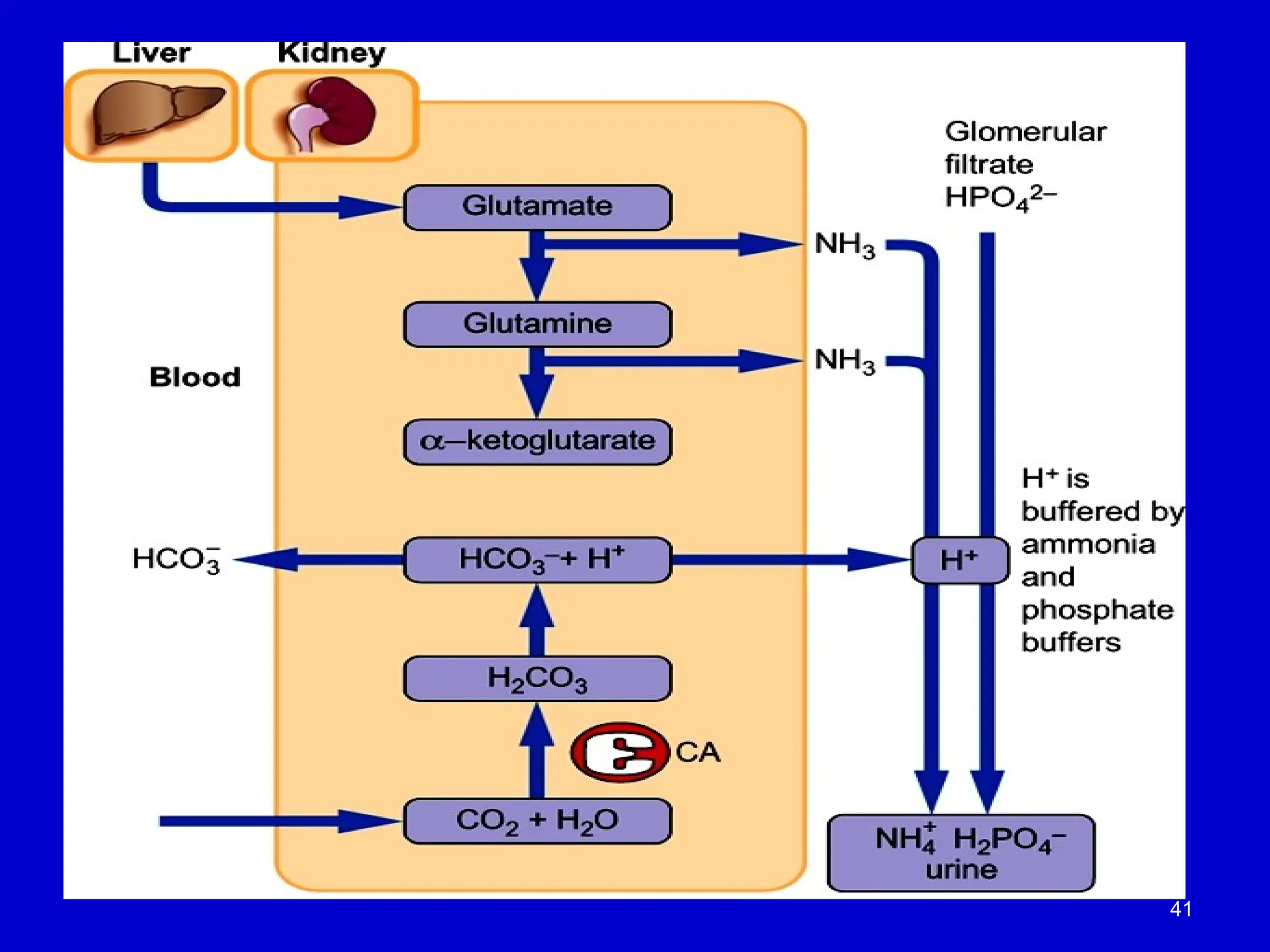
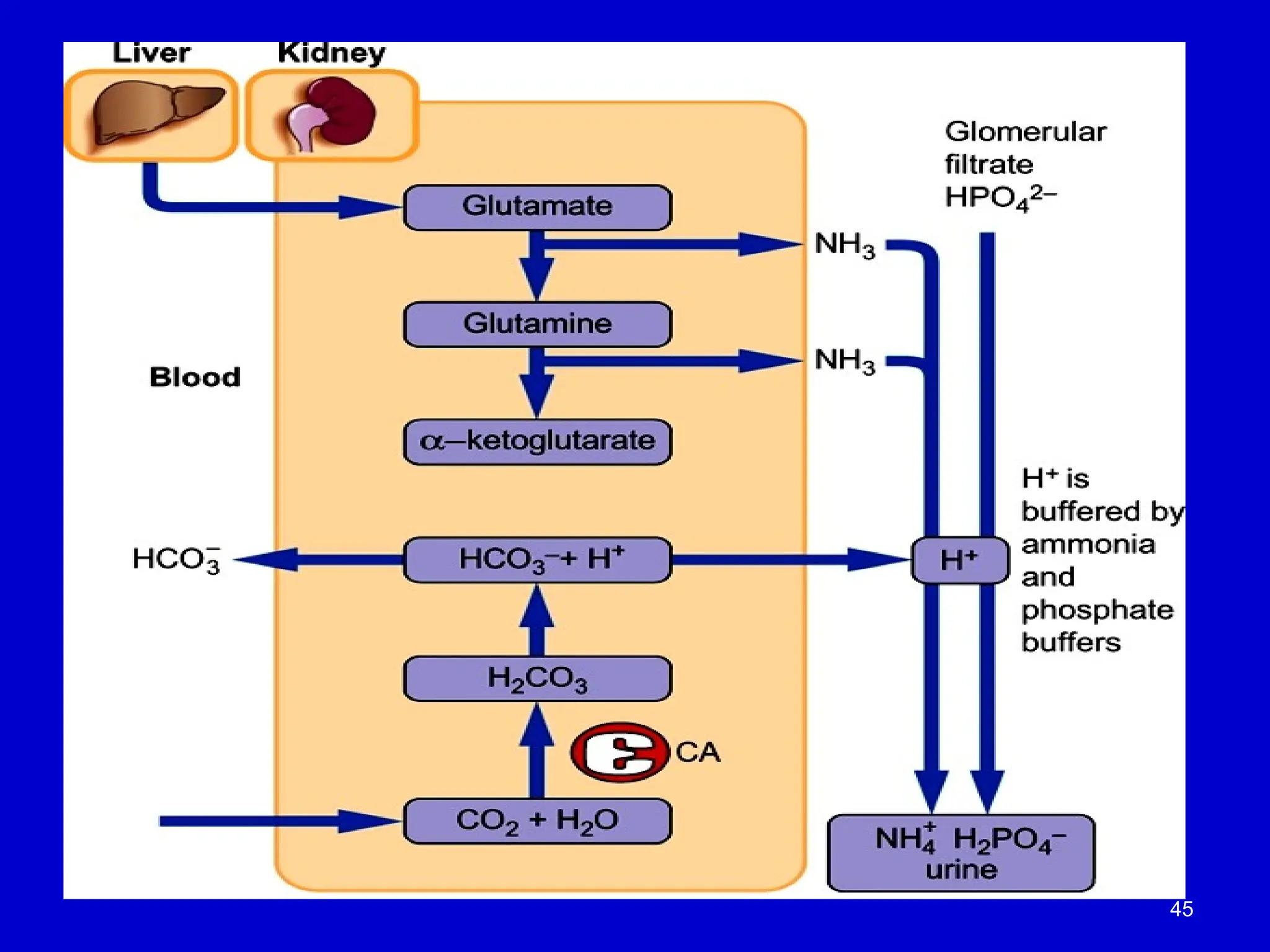
• Phosphate and Ammonia Buffering:
• In the distal tubule, bicarbonate has already been reabsorbed, so hydrogen ions are
buffered by:
• Phosphate ions (present in the filtrate), which trap hydrogen ions.
• Ammonia (NH )
₃ , synthesized by the proximal tubules, which also helps buffer hydrogen ions.
• Excretion of Hydrogen Ions:
• The buffered hydrogen ions (H ) are
⁺ excreted in the urine as part of the acid-base
regulation.
• Clinical Relevance:
• This process is essential for excreting excess acid from the body and for maintaining pH
homeostasis.
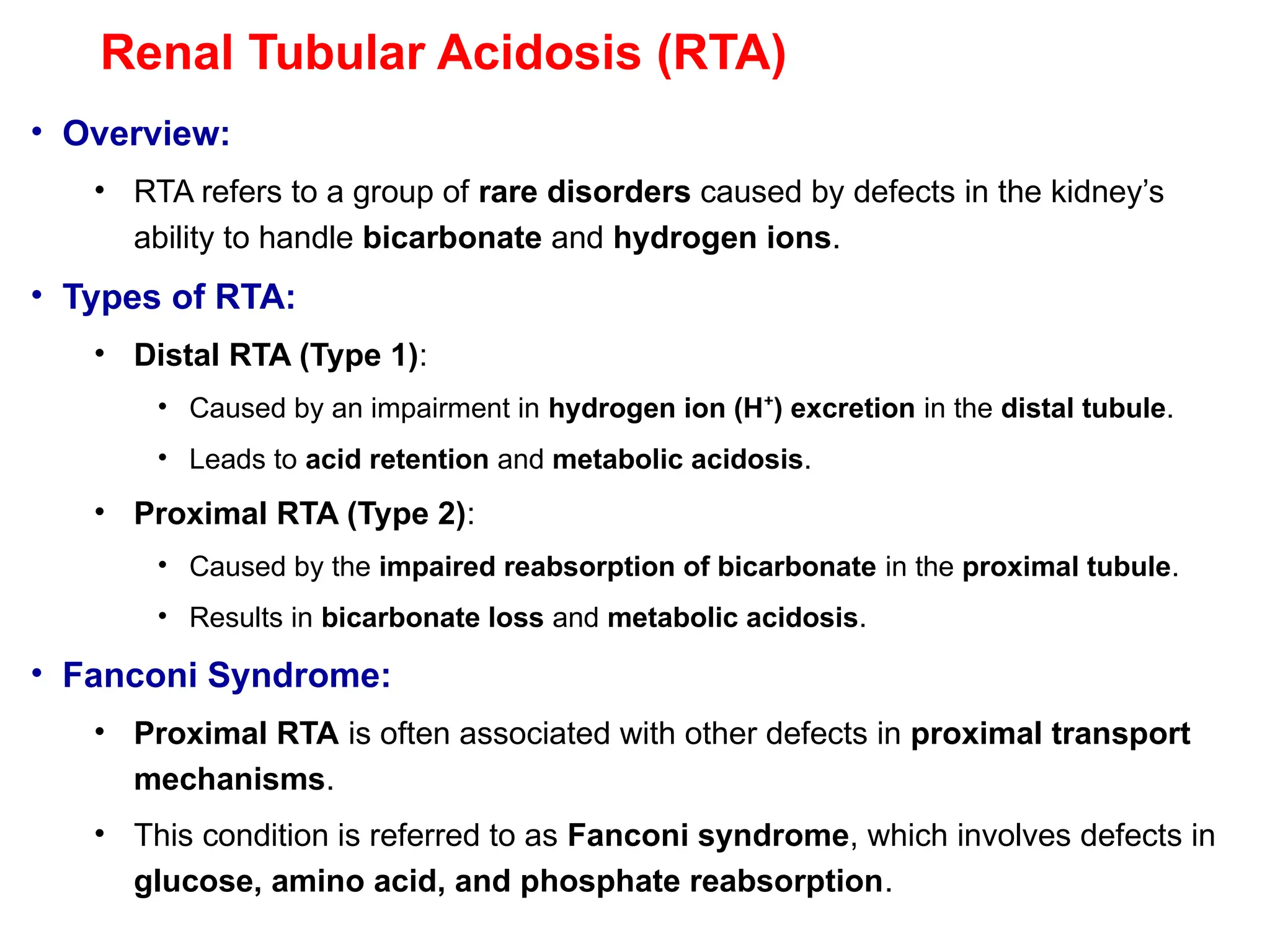
Renal Tubular Acidosis(RTA)
• Overview:
• RTA refers to a group of rare disorders caused by defects in the kidney’s
ability to handle bicarbonate and hydrogen ions.
• Types of RTA:
• Distal RTA (Type 1):
• Caused by an impairment in hydrogen ion (H ) excretion
⁺ in the distal tubule.
• Leads to acid retention and metabolic acidosis.
• Proximal RTA (Type 2):
• Caused by the impaired reabsorption of bicarbonate in the proximal tubule.
• Results in bicarbonate loss and metabolic acidosis.
• Fanconi Syndrome:
• Proximal RTA is often associated with other defects in proximal transport
mechanisms.
• This condition is referred to as Fanconi syndrome, which involves defects in
glucose, amino acid, and phosphate reabsorption.
44.
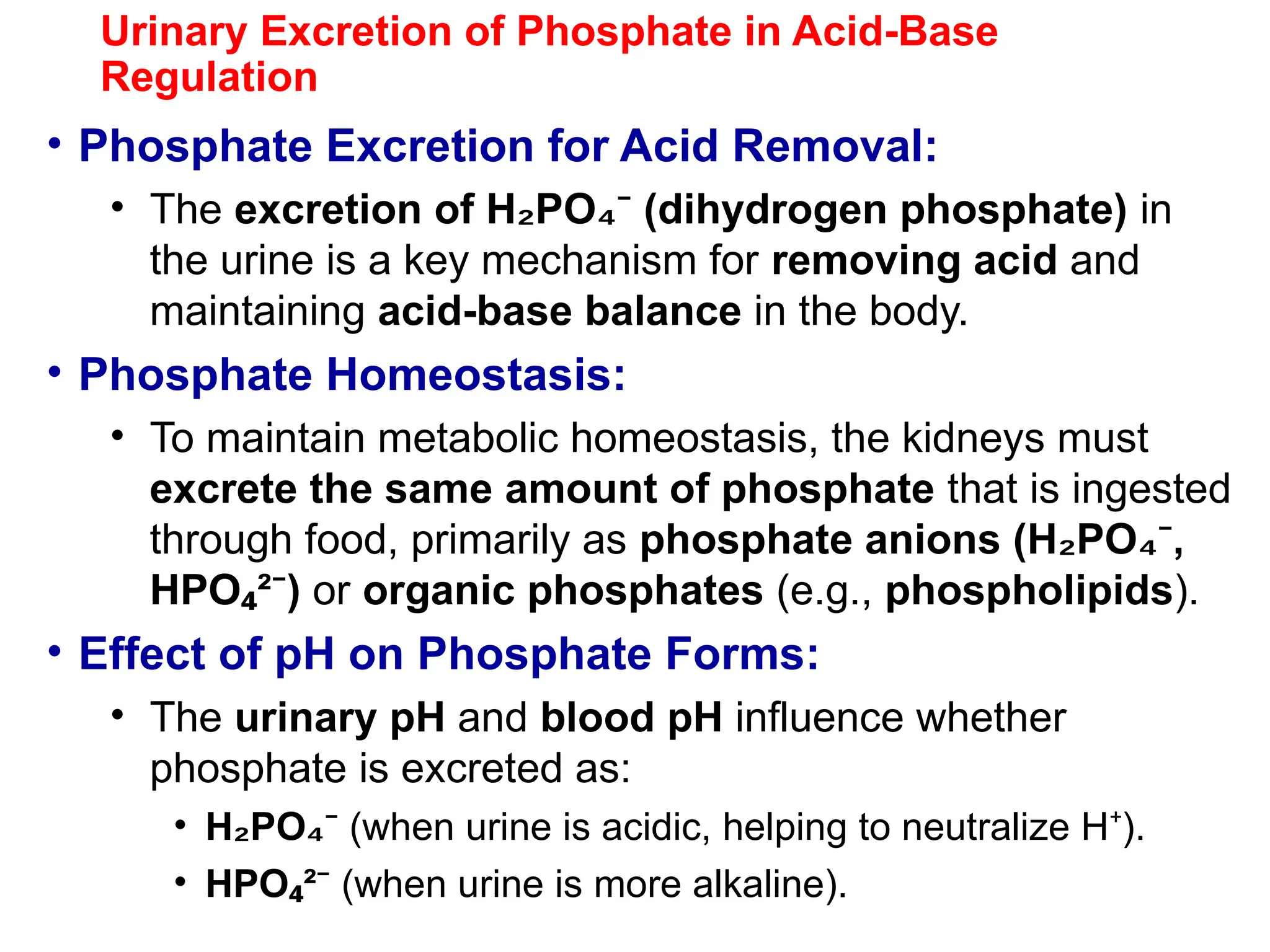
Urinary Excretion ofPhosphate in Acid-Base
Regulation
• Phosphate Excretion for Acid Removal:
• The excretion of H PO (dihydrogen phosphate)
₂ ₄⁻ in
the urine is a key mechanism for removing acid and
maintaining acid-base balance in the body.
• Phosphate Homeostasis:
• To maintain metabolic homeostasis, the kidneys must
excrete the same amount of phosphate that is ingested
through food, primarily as phosphate anions (H PO ,
₂ ₄⁻
HPO ² )
₄ ⁻ or organic phosphates (e.g., phospholipids).
• Effect of pH on Phosphate Forms:
• The urinary pH and blood pH influence whether
phosphate is excreted as:
• H PO
₂ ₄⁻ (when urine is acidic, helping to neutralize H ).
⁺
• HPO ²
₄ ⁻ (when urine is more alkaline).
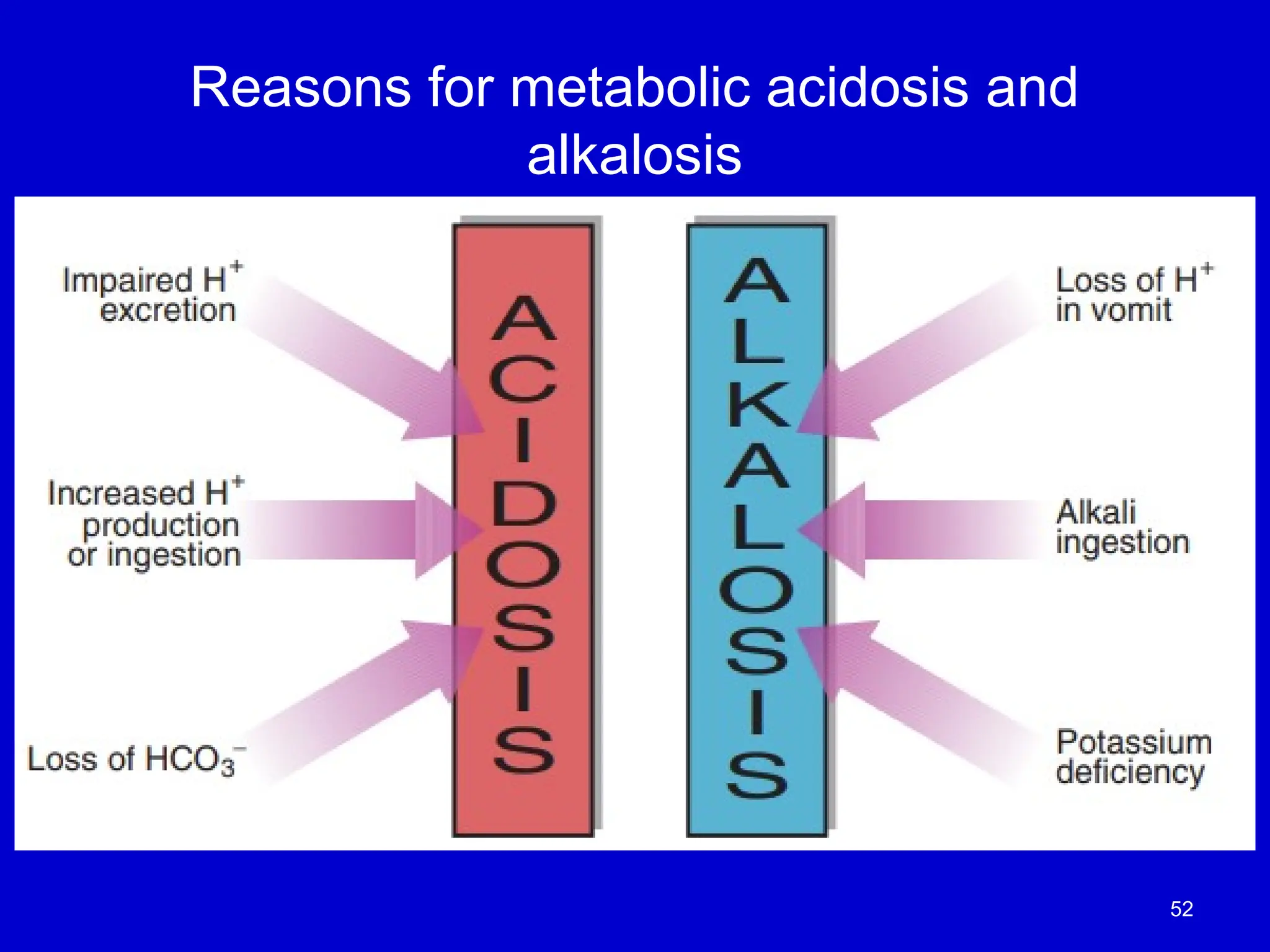
Classification of Acid-BaseDisorders
• Acidosis vs Alkalosis:
• Acidosis: Accumulation of hydrogen ions (H )
⁺
• Alkalosis: Decrease in hydrogen ion concentration
• Terms:
• Acidemia: Blood pH < 7.35 (due to acidosis)
• Alkalemia: Blood pH > 7.45 (due to alkalosis)
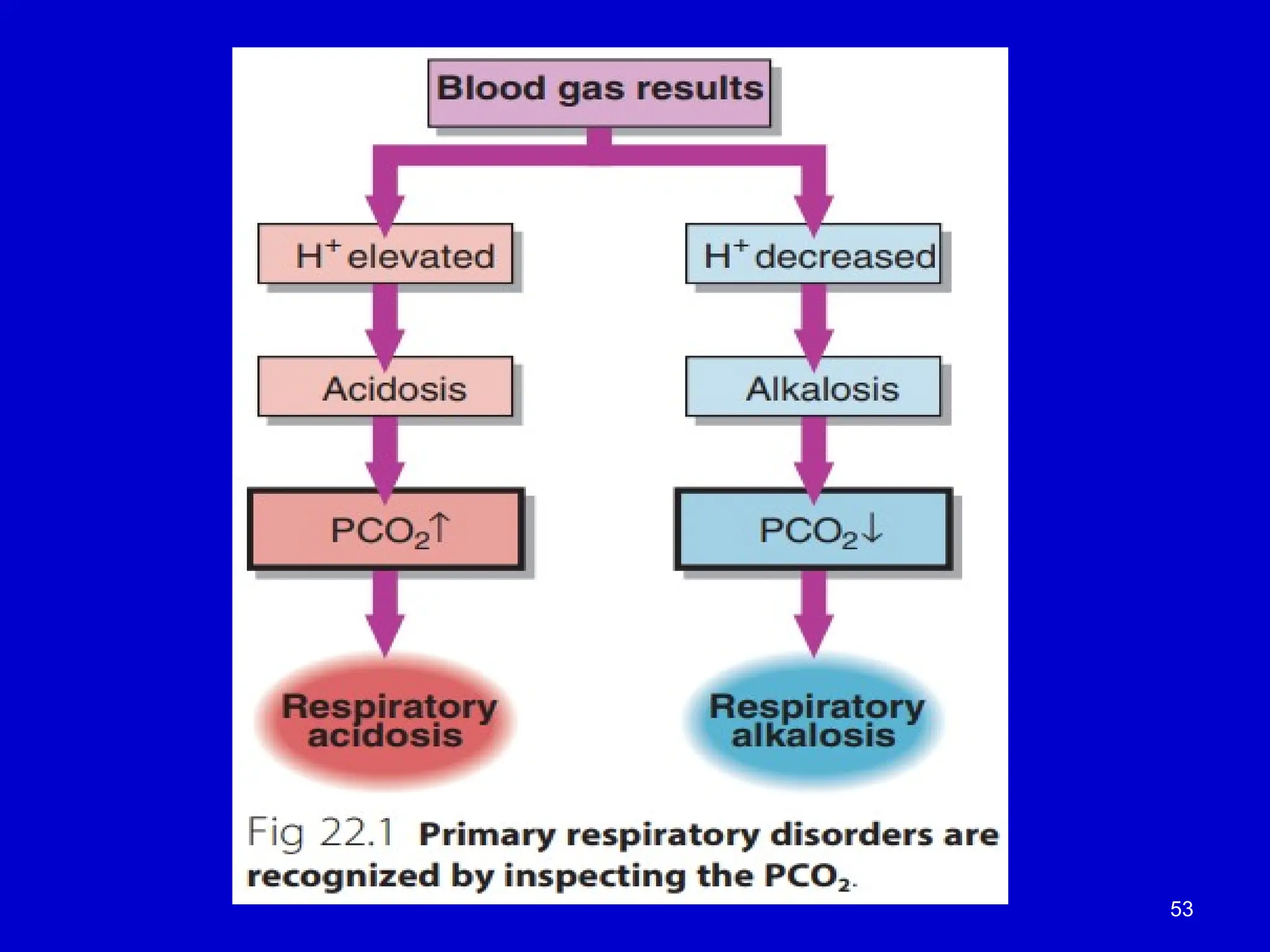
• Types of Disorders:
1.Respiratory Acidosis: Due to impaired CO elimination (e.g., hypoventilation)
₂
2.Metabolic Acidosis: Due to excess acid production or bicarbonate loss (e.g.,
kidney failure)
3.Respiratory Alkalosis: Due to excessive CO loss (e.g., hyperventilation)
₂
4.Metabolic Alkalosis: Due to excessive bicarbonate or loss of acid (e.g.,
vomiting)
• ⚖️Proper identification of the disorder helps in targeted
treatment and management.
49.
Respiratory and MetabolicComponents of
Acid-Base Balance
• Role of Lungs and Kidneys:
• The lungs and kidneys work together to maintain a stable hydrogen
ion (H )
⁺ concentration and preserve blood pH.
• The lungs are responsible for the respiratory component, and the
kidneys are responsible for the metabolic component of acid-base
balance.
• Interrelationship Between Components:
• The respiratory component regulates carbon dioxide (CO )
₂ levels
in the blood, while the metabolic component regulates bicarbonate
(HCO )
₃⁻ .
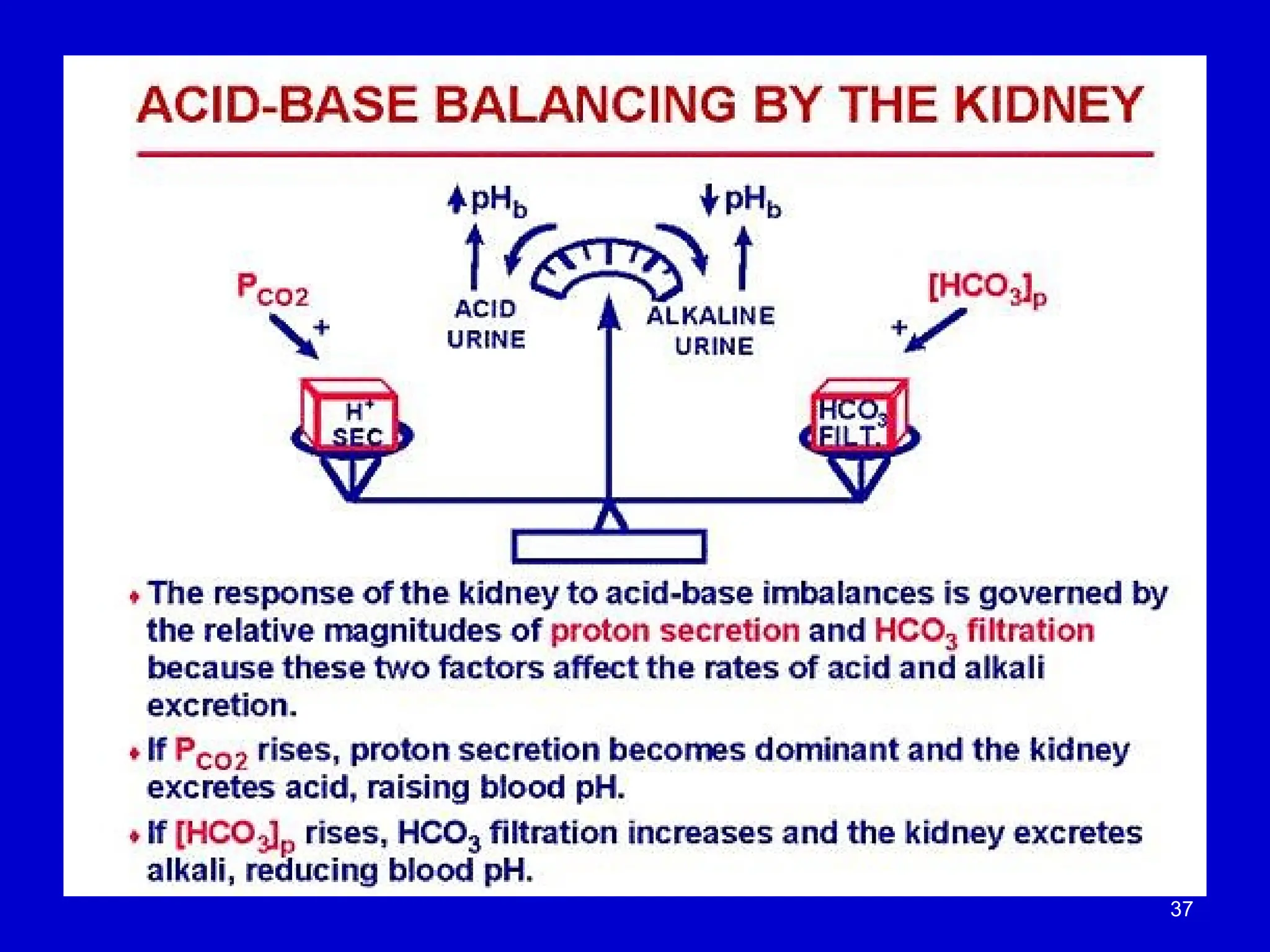
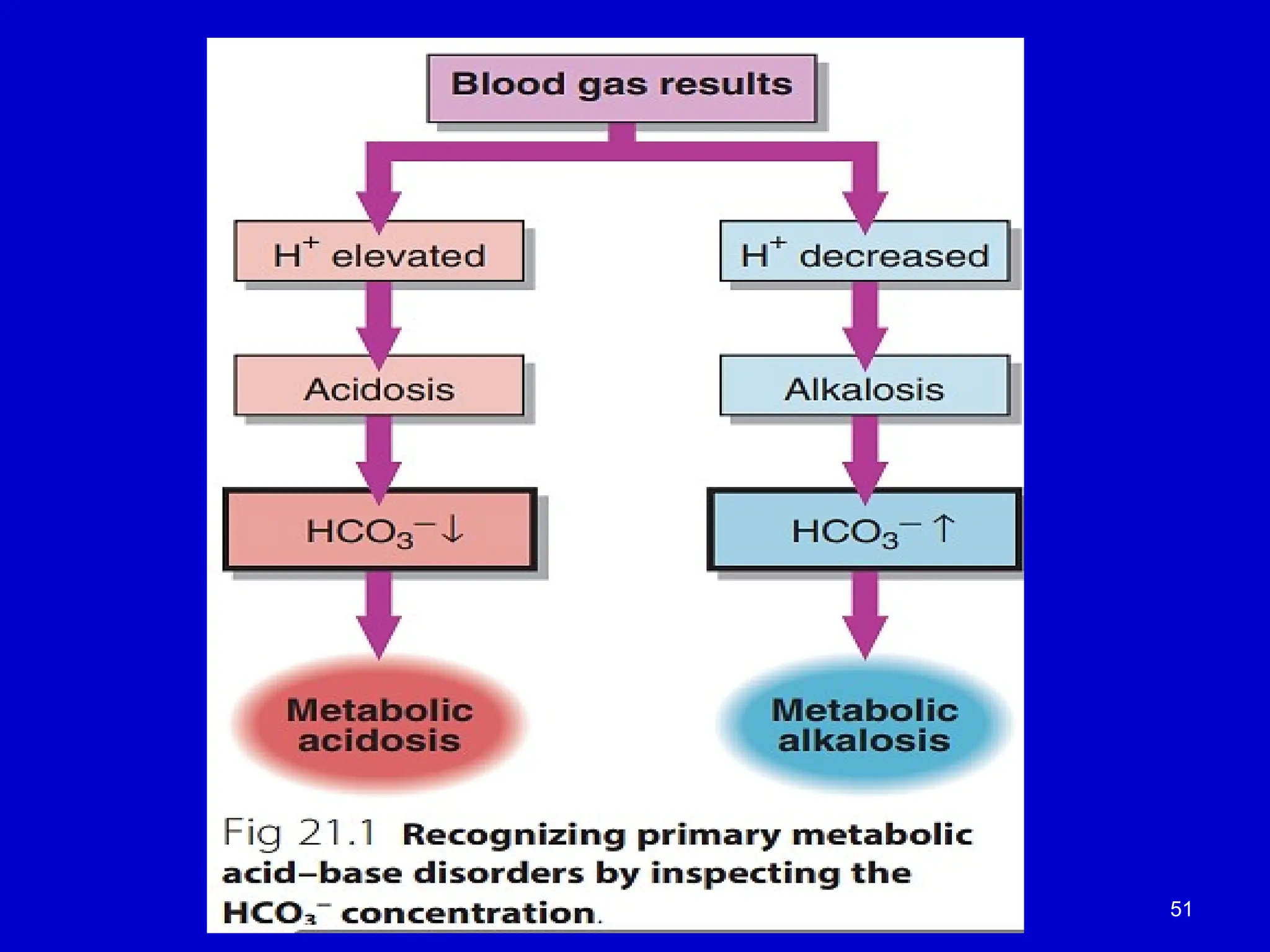
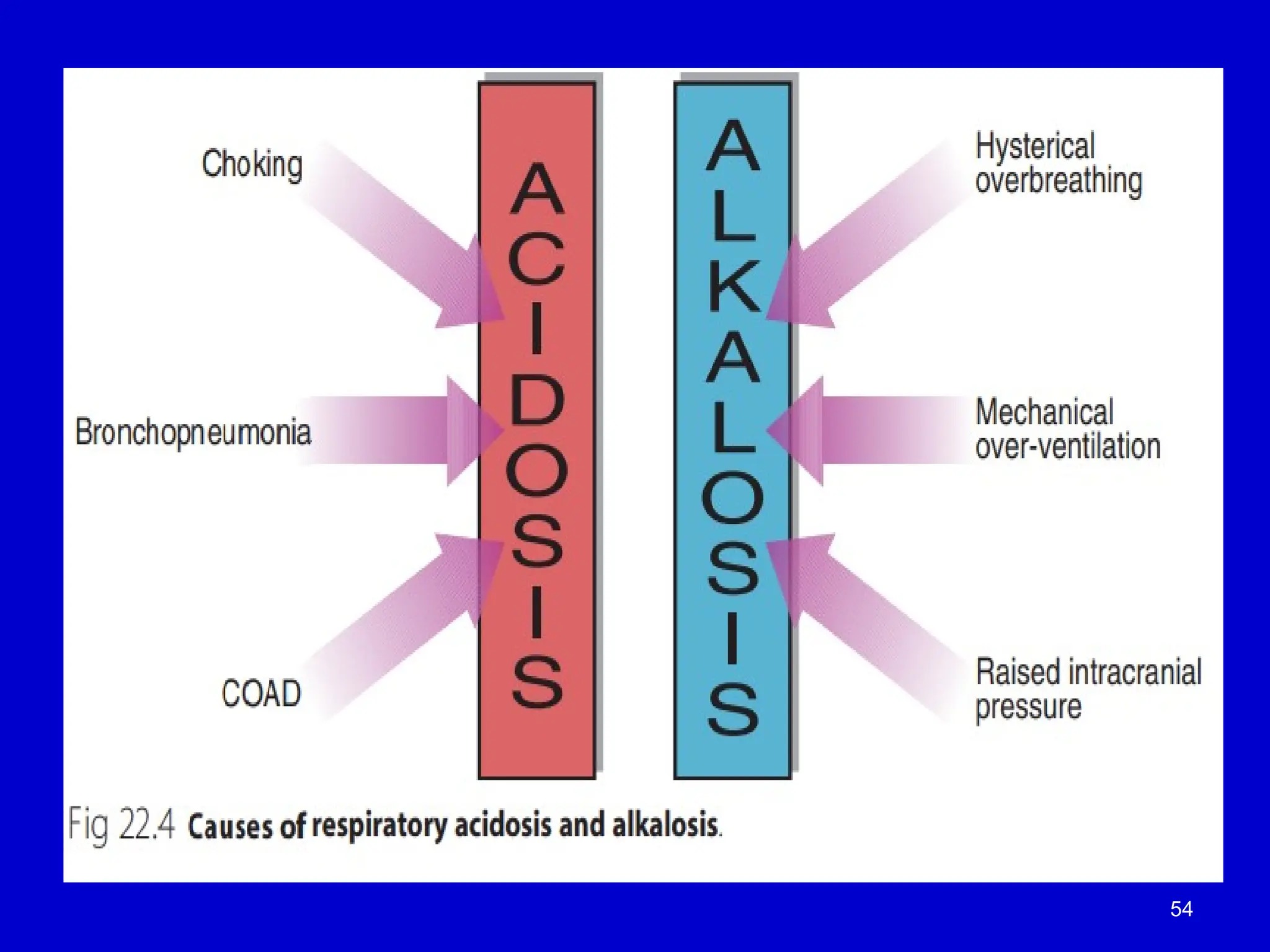
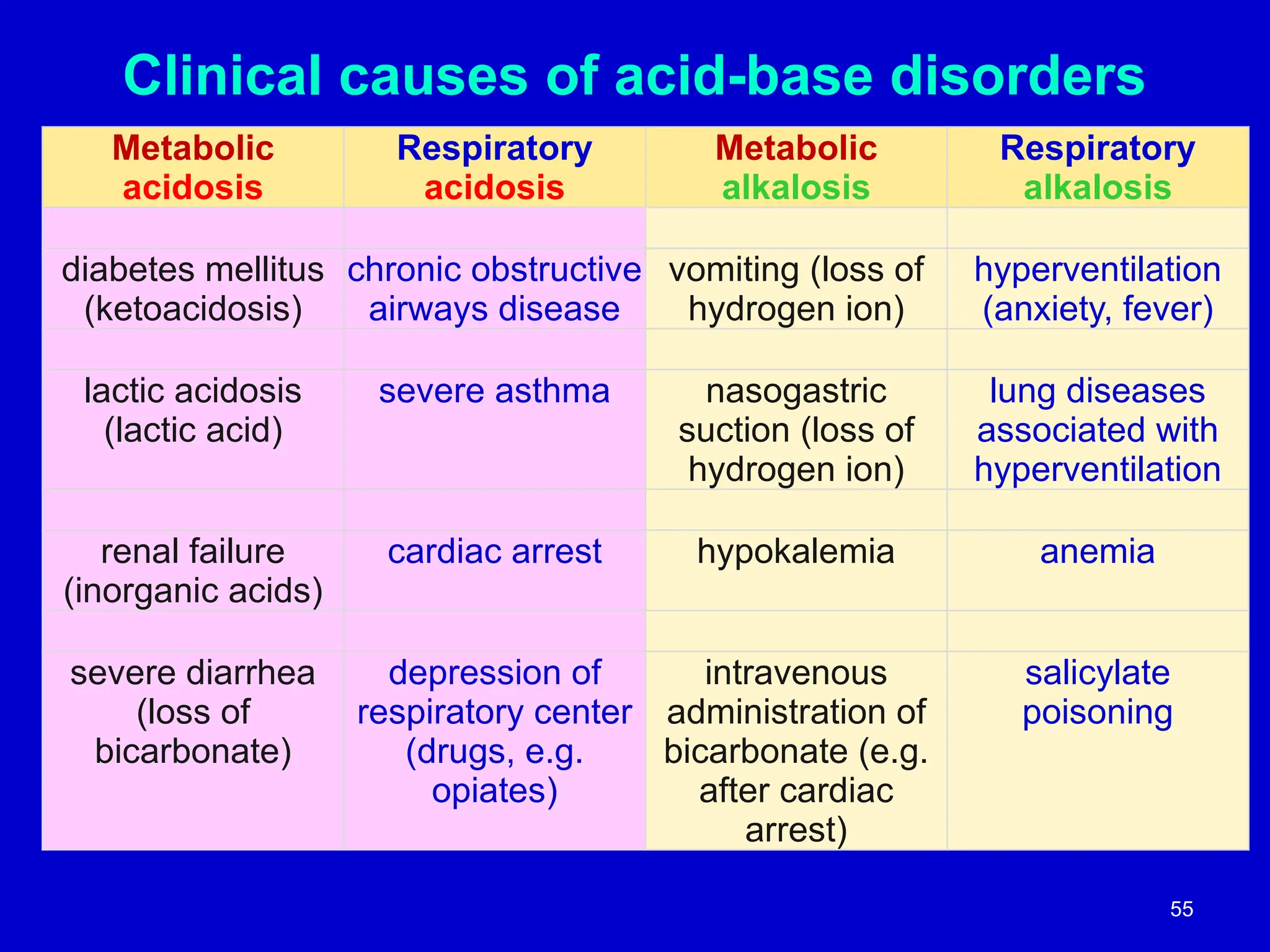
Clinical causes ofacid-base disorders
Metabolic
acidosis
Respiratory
acidosis
Metabolic
alkalosis
Respiratory
alkalosis
diabetes mellitus
(ketoacidosis)
chronic obstructive
airways disease
vomiting (loss of
hydrogen ion)
hyperventilation
(anxiety, fever)
lactic acidosis
(lactic acid)
severe asthma nasogastric
suction (loss of
hydrogen ion)
lung diseases
associated with
hyperventilation
renal failure
(inorganic acids)
cardiac arrest hypokalemia anemia
severe diarrhea
(loss of
bicarbonate)
depression of
respiratory center
(drugs, e.g.
opiates)
intravenous
administration of
bicarbonate (e.g.
after cardiac
arrest)
salicylate
poisoning
55
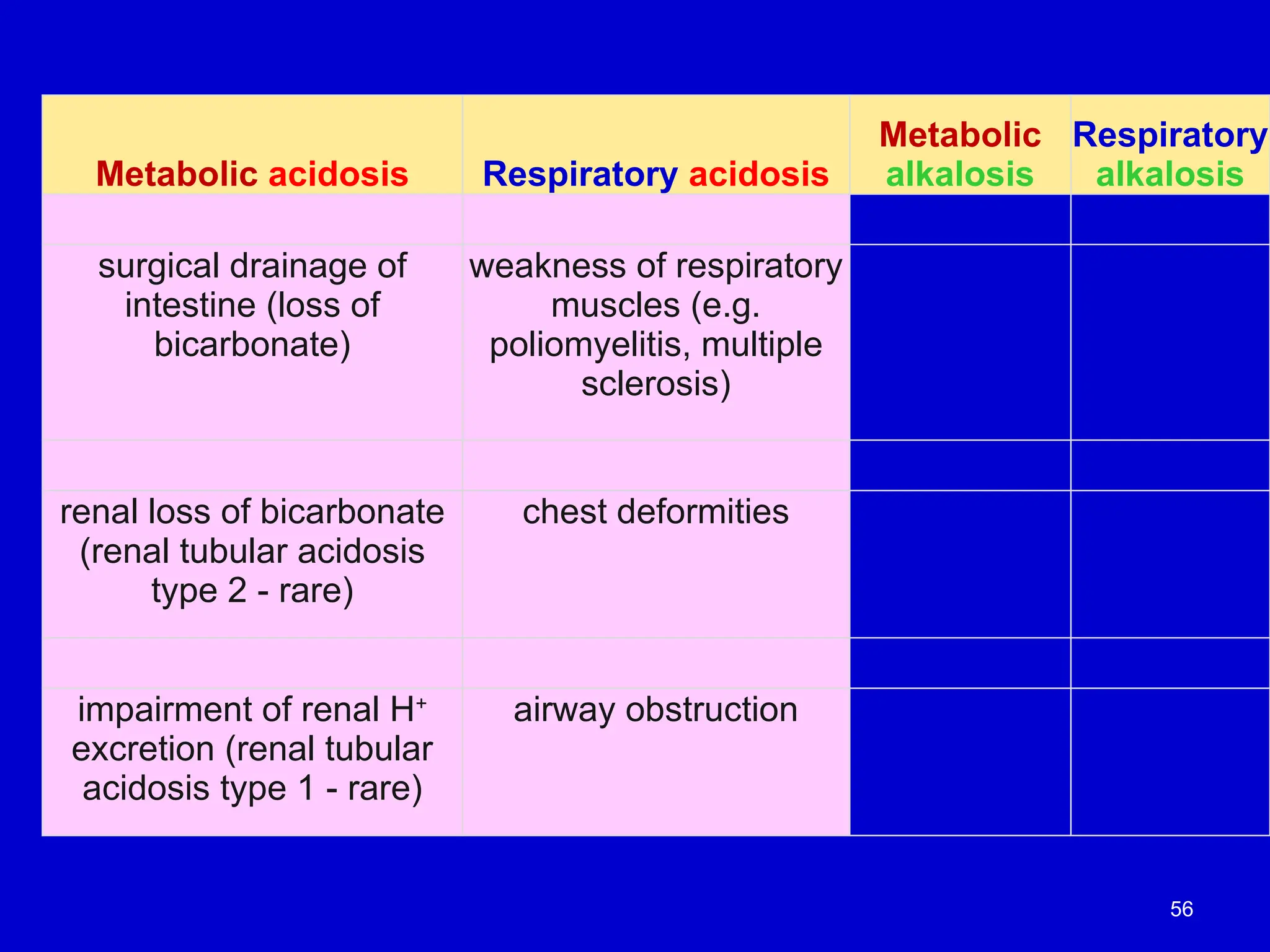
56.
Metabolic acidosis Respiratoryacidosis
Metabolic
alkalosis
Respiratory
alkalosis
surgical drainage of
intestine (loss of
bicarbonate)
weakness of respiratory
muscles (e.g.
poliomyelitis, multiple
sclerosis)
renal loss of bicarbonate
(renal tubular acidosis
type 2 - rare)
chest deformities
impairment of renal H+
excretion (renal tubular
acidosis type 1 - rare)
airway obstruction
56
57.
Renal Failure andMetabolic Acidosis
• Impaired Excretion of Nonvolatile Acids:
• Renal failure impairs the kidneys’ ability to excrete nonvolatile acids, leading
to metabolic acidosis.
• This occurs because the kidneys are unable to effectively remove hydrogen
ions and reclaim bicarbonate.
• Causes of Renal Failure:
• Inadequate Kidney Perfusion:
• Conditions like trauma, shock, or dehydration reduce blood flow to the
kidneys, impairing their function.
• Intrinsic Kidney Disease:
• Diseases such as glomerulonephritis (an inflammatory reaction in renal
tissue) can also lead to renal failure.
• Excessive Bicarbonate Loss:
• Bicarbonate loss contributes to metabolic acidosis, often due to:
• Defective renal reabsorption of bicarbonate.
• Loss of bicarbonate in intestinal fluid during conditions like severe
diarrhea or post-surgical drainage following bowel surgery.
58.
Alkalosis and ItsCauses
• Overview of Alkalosis:
• Alkalosis is rarer than acidosis, but it still plays a role in acid-base imbalances.
• Types of Alkalosis:
• Respiratory Alkalosis:
• Often caused by hyperventilation during conditions such as:
• Exercise, Anxiety attacks, Fever, Pregnancy
• Metabolic Alkalosis:
• Commonly associated with low potassium concentrations in plasma
(hypokalemia).
• Cellular buffering mechanisms lead to the movement of hydrogen ions (H )
⁺
in and out of cells, influencing potassium ion exchange.
• Alkalosis can lead to hypokalemia, and hypokalemia can cause alkalosis.
• Causes of Severe Metabolic Alkalosis:
• Massive loss of hydrogen ions through:
• Vomiting (loss of stomach acid).
• Nasogastric suction after surgery.
• Excess bicarbonate administration, such as during:
• Cardiac arrest resuscitation, leading to overcorrection of acid-base balance.
59.
Aspirin (Acetylsalicylic Acid)and Acid-Base Balance
• Conversion to Salicylic Acid:
• Aspirin is rapidly converted to salicylic acid in the body.
• Initial Effect: Respiratory Alkalosis:
• The initial effect of aspirin is respiratory alkalosis, which occurs due to:
• Stimulation of the central respiratory control center in the medulla.
• This causes hyperventilation (increased breathing rate) and exhalation of CO₂, leading to a
decrease in blood CO levels.
₂
• Subsequent Effect: Metabolic Acidosis:
• Following the respiratory alkalosis, a metabolic acidosis develops, caused by:
• Dissociation of salicylic acid into salicylate and hydrogen ions (H )
⁺ .
• The reaction:
• Salicylic acid ↔ Salicylate + H
⁻ ⁺ (pKa ≈ 3.5).
• This increase in H concentration
⁺ contributes to metabolic acidosis.
• Clinical Relevance:
• The dual effects of aspirin (respiratory alkalosis followed by metabolic acidosis) require
careful monitoring, especially in cases of aspirin overdose or chronic usage.
• Metabolic acidosis from aspirin toxicity can be severe and requires medical
intervention.
60.
Salicylate Effects onMetabolism and Renal Function
• Interference with Mitochondrial ATP Production:
• Salicylate acts as an uncoupler of mitochondrial ATP production, leading to:
• Increased generation of CO₂.
• Stimulation of glycolysis, resulting in the accumulation of lactate and other
organic acids in the blood.
• Increased Blood Acidity:
• The accumulation of lactate and organic acids contributes to metabolic
acidosis.
• Impact on Renal Function:
• Salicylate toxicity may impair renal function, leading to:
• Reduced ability to excrete strong acids, such as sulfuric acid and phosphoric
acid, which are produced from normal metabolism.
• This further contributes to the acid load in the body.
• Clinical Implications:
• The uncoupling effect of salicylate and its impact on renal function
exacerbate metabolic acidosis in cases of aspirin overdose or toxicity,
requiring urgent medical treatment to restore acid-base balance and renal
function.
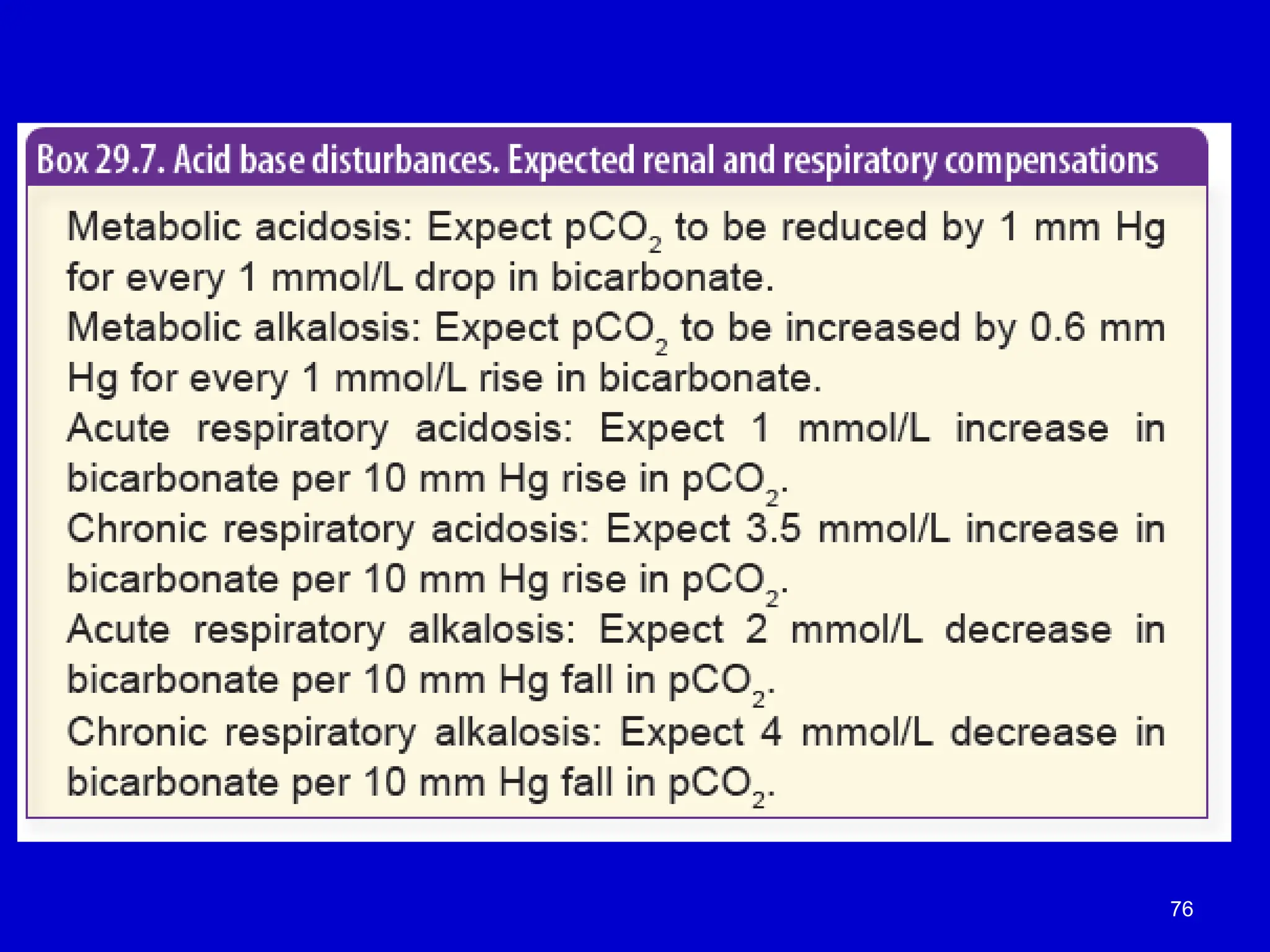
61.
Compensation in Acid-BaseDisorders
• Definition:
• Compensation is a homeostatic response by the body to restore the
HCO /H CO ratio
₃⁻ ₂ ₃ (bicarbonate to carbonic acid ratio) in the blood.
• Types of Compensation:
• Ventilatory Compensation:
• Response to metabolic abnormalities (e.g., metabolic acidosis or alkalosis).
• The lungs adjust the rate of CO (carbon dioxide) exhalation
₂ to either increase or
decrease CO levels in the blood, helping to normalize pH.
₂
• Metabolic Compensation:
• Response to respiratory abnormalities (e.g., respiratory acidosis or alkalosis).
• The kidneys adjust the reabsorption or excretion of bicarbonate (HCO )
₃⁻ to help
balance the blood's pH.
• Clinical Relevance:
• Proper compensation is crucial in maintaining normal blood pH (7.35–7.45).
• Incomplete or impaired compensation can lead to chronic acid-base
imbalances, affecting organ function.
62.
Primary Alteration inCO2
Respiratory Acidosis (10
CO2 excess)
CO2 + H2O ↔ H2CO3↔ H+
+ HCO3- =pH
Blood
Causes
Hypoventilation (CO2 retention)
- airway obstruction
- depression of respiratory center
- neuromuscular disease
pH = pK + log[HCO3
-
]
[Pco2]
Ratio < 20
62
63.
Compensation in RespiratoryAcidosis
• slowly, kidney
– increases H+
excretion
– increases HCO3
-
regeneration
• Net effect: increase of plasma [HCO3
-
]
[HCO3
-
]
[Pco2]
pH moves up towards normal.
63
Compensation in RespiratoryAlkalosis
• Slowly, several days
– renal H+
excretion decreased
• Net effect is to increase renal HCO3
-
loss
[HCO3
-
]
[Pco2]
pH moves down towards normal.
65
Compensation in MetabolicAcidosis
• Respiratory center is stimulated causing
increased loss of CO2
• Kidney
– increases the excretion of acid
– increases reabsorption of [HCO3
-
]
[HCO3
-
]
[Pco2]
pH moves up towards normal. 67
Compensation in MetabolicAlkalosis
• Effect is to decrease the respiratory center
causing a retention of CO2 -minimal
• Kidney
– forms less ammonia
– renal H+
excretion decreased
– Decreases reabsorption of [HCO3
-
]
[HCO3
-
]
[Pco2]
pH moves down towards normal.
69
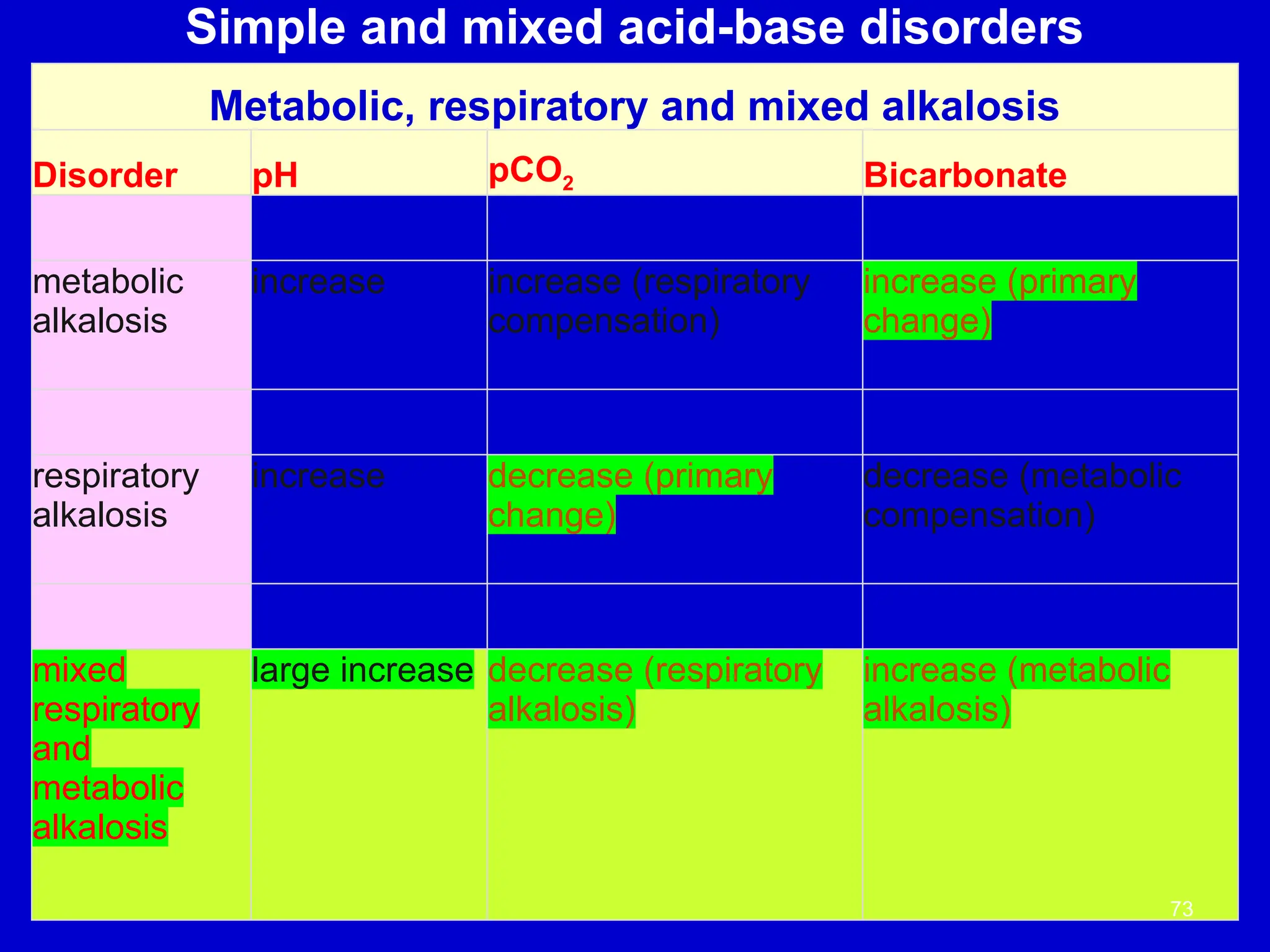
70.
The Four CardinalAcid Base Disorders
M acidosis
M alkalosis
R acidosis
R alkalosis
Disorder pH pCO2 [HCO3
-
]
70
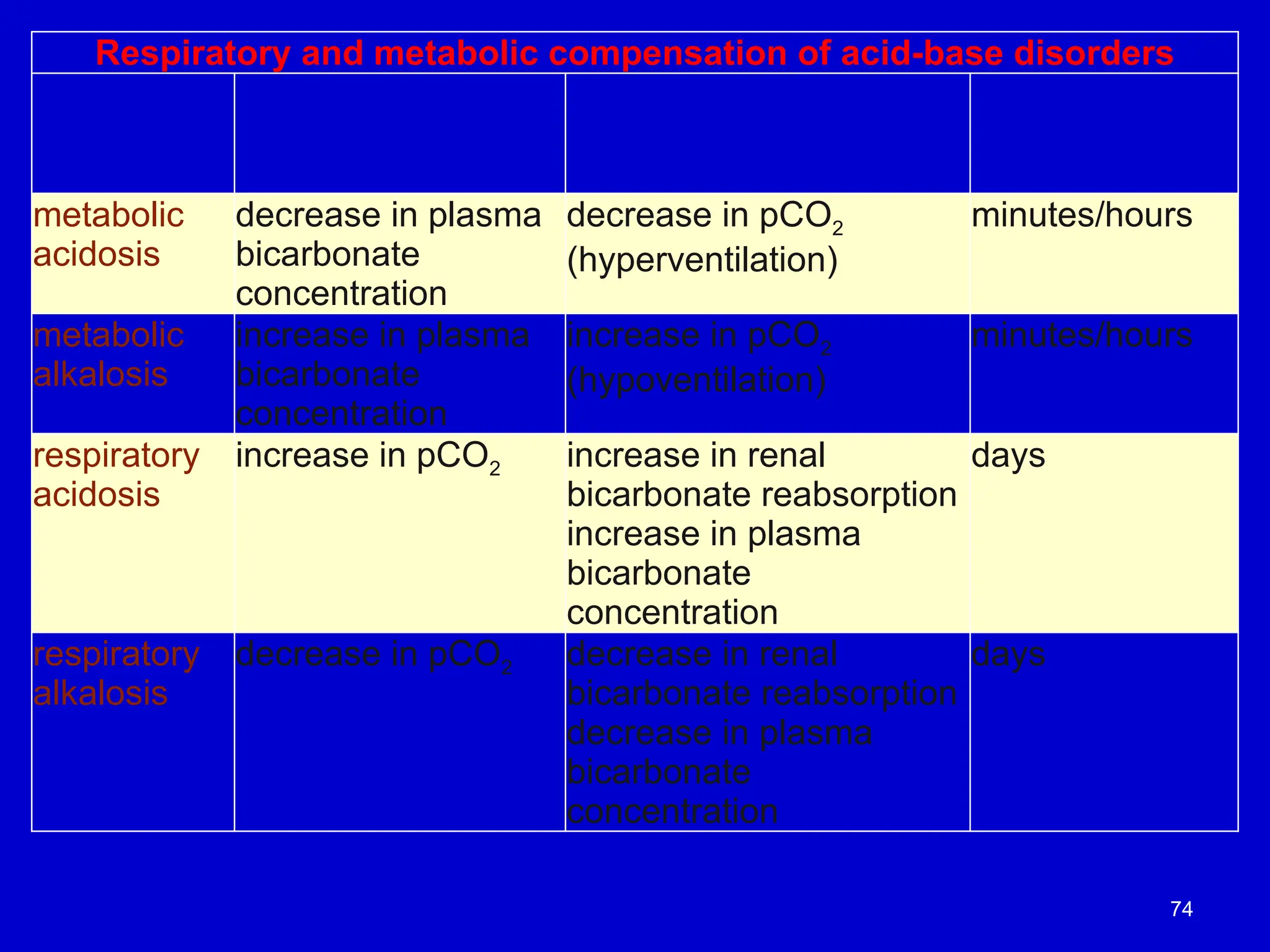
Respiratory and metaboliccompensation of acid-base disorders
Acid-base
disorder
Primary change Compensatory change Timescale of
compensatory
change
metabolic
acidosis
decrease in plasma
bicarbonate
concentration
decrease in pCO2
(hyperventilation)
minutes/hours
metabolic
alkalosis
increase in plasma
bicarbonate
concentration
increase in pCO2
(hypoventilation)
minutes/hours
respiratory
acidosis
increase in pCO2 increase in renal
bicarbonate reabsorption
increase in plasma
bicarbonate
concentration
days
respiratory
alkalosis
decrease in pCO2 decrease in renal
bicarbonate reabsorption
decrease in plasma
bicarbonate
concentration
days
74
Anion Gap
Anions
• 80%of plasma anions is Cl-
& HCO3
-
• 20% is made of “unmeasured anions”
– (urate, SO4
2-
, PO4
2-
, lactate, ethanol, etc)
Cations
• > 90% is provided by Na+
& K+
• 10% includes Ca2+
, Mg2+
78
79.
Anion Gap
is thedifference between the total conc. of
measured cations and that of measured anions
Anion Gap (A-) = ([Na+
] + [K+
]) – ([Cl-
] + [HCO3
-
])
RR: 12 - 20 mmol/l
79
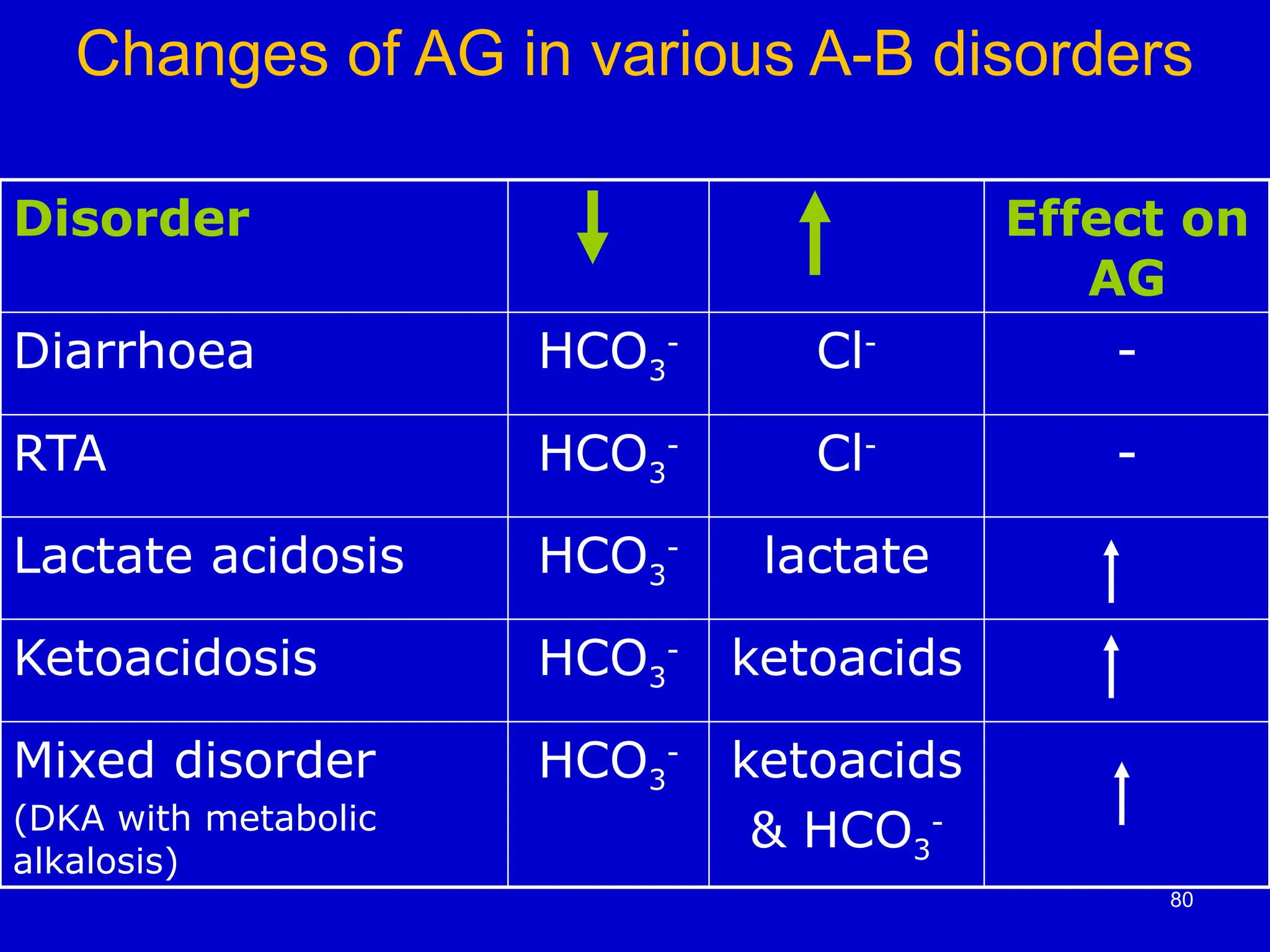
80.
Changes of AGin various A-B disorders
Disorder Effect on
AG
Diarrhoea HCO3
-
Cl-
-
RTA HCO3
-
Cl-
-
Lactate acidosis HCO3
-
lactate
Ketoacidosis HCO3
-
ketoacids
Mixed disorder
(DKA with metabolic
alkalosis)
HCO3
-
ketoacids
& HCO3
-
80
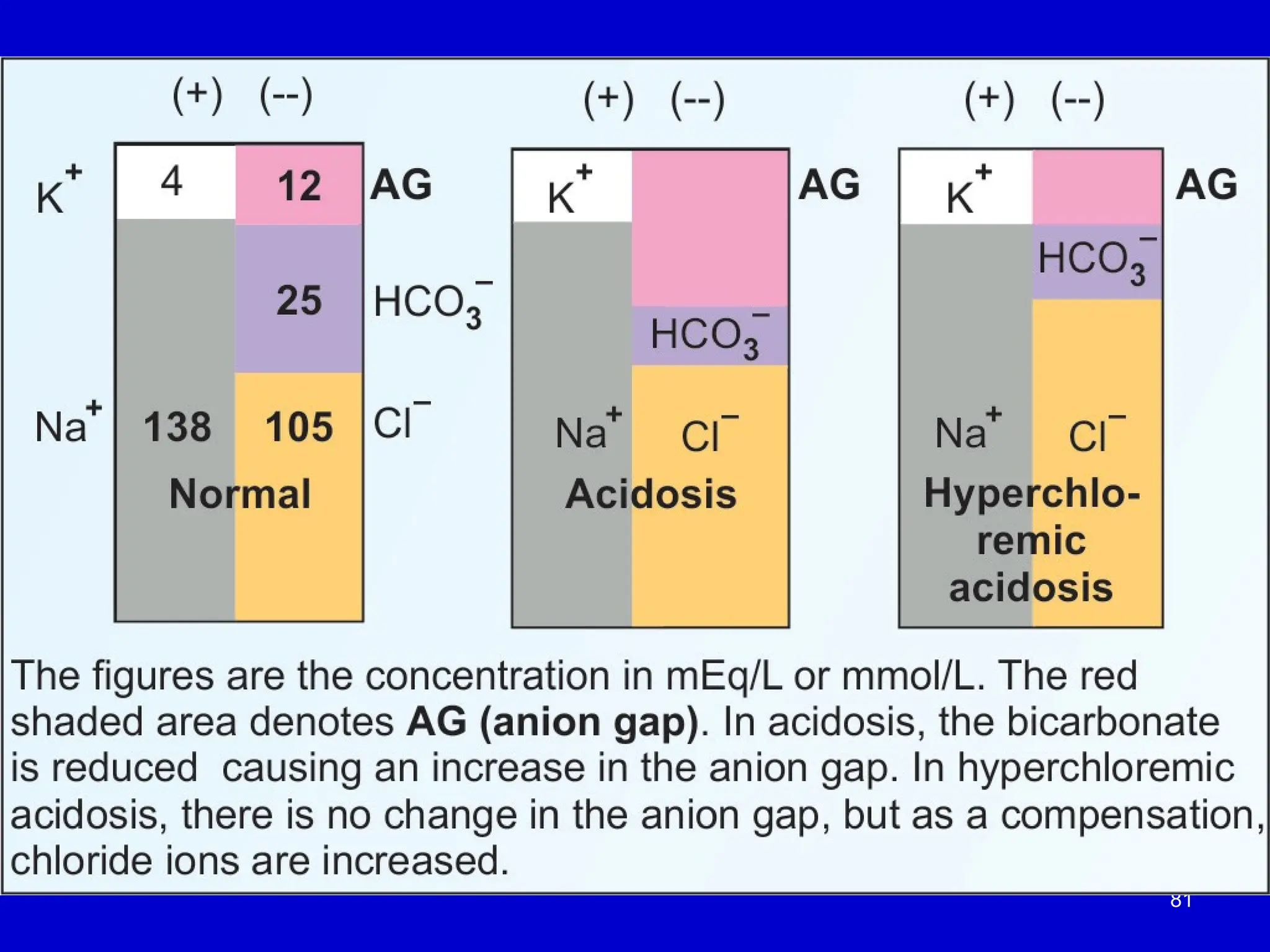
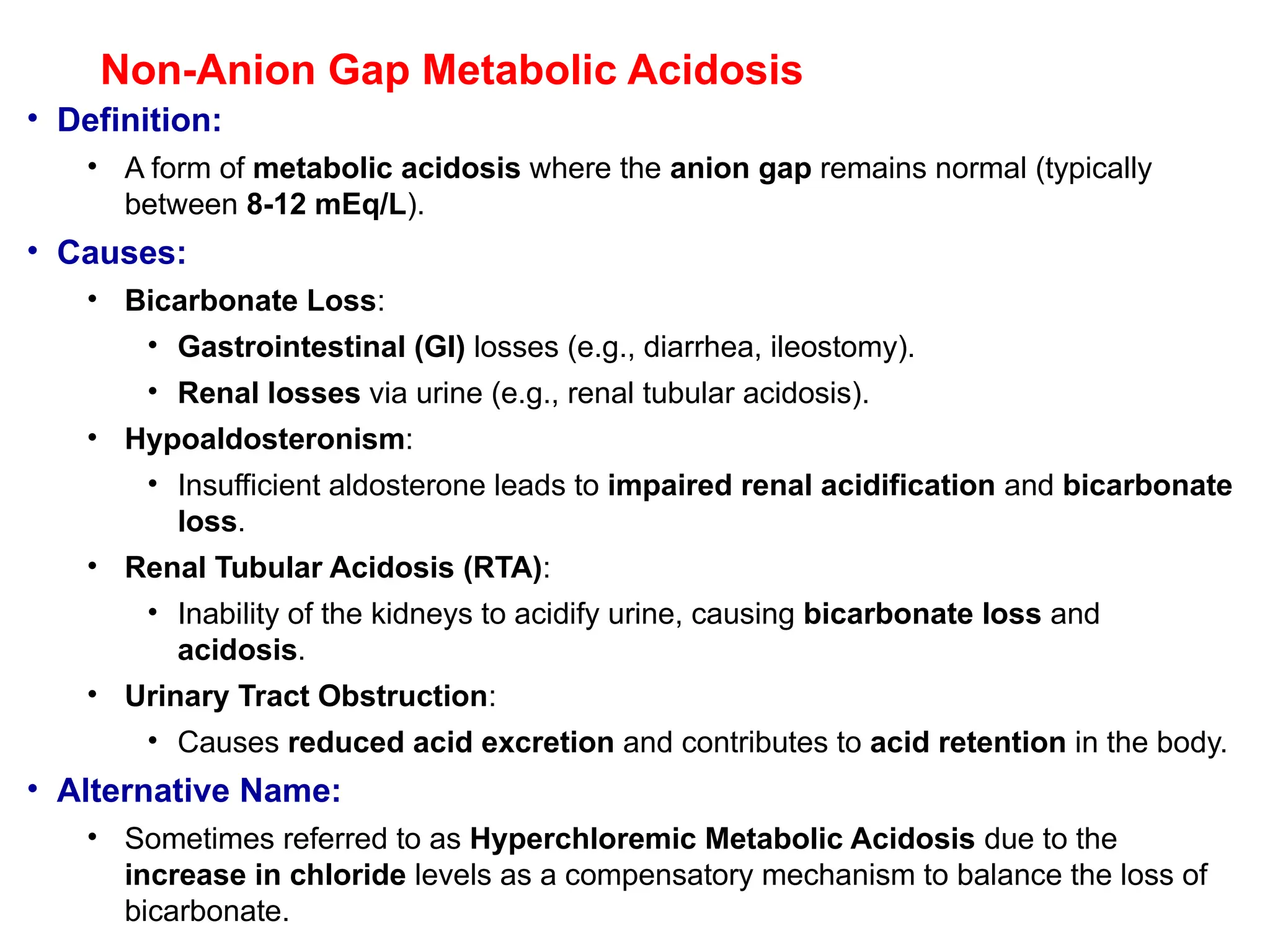
Non-Anion Gap MetabolicAcidosis
• Definition:
• A form of metabolic acidosis where the anion gap remains normal (typically
between 8-12 mEq/L).
• Causes:
• Bicarbonate Loss:
• Gastrointestinal (GI) losses (e.g., diarrhea, ileostomy).
• Renal losses via urine (e.g., renal tubular acidosis).
• Hypoaldosteronism:
• Insufficient aldosterone leads to impaired renal acidification and bicarbonate
loss.
• Renal Tubular Acidosis (RTA):
• Inability of the kidneys to acidify urine, causing bicarbonate loss and
acidosis.
• Urinary Tract Obstruction:
• Causes reduced acid excretion and contributes to acid retention in the body.
• Alternative Name:
• Sometimes referred to as Hyperchloremic Metabolic Acidosis due to the
increase in chloride levels as a compensatory mechanism to balance the loss of
bicarbonate.
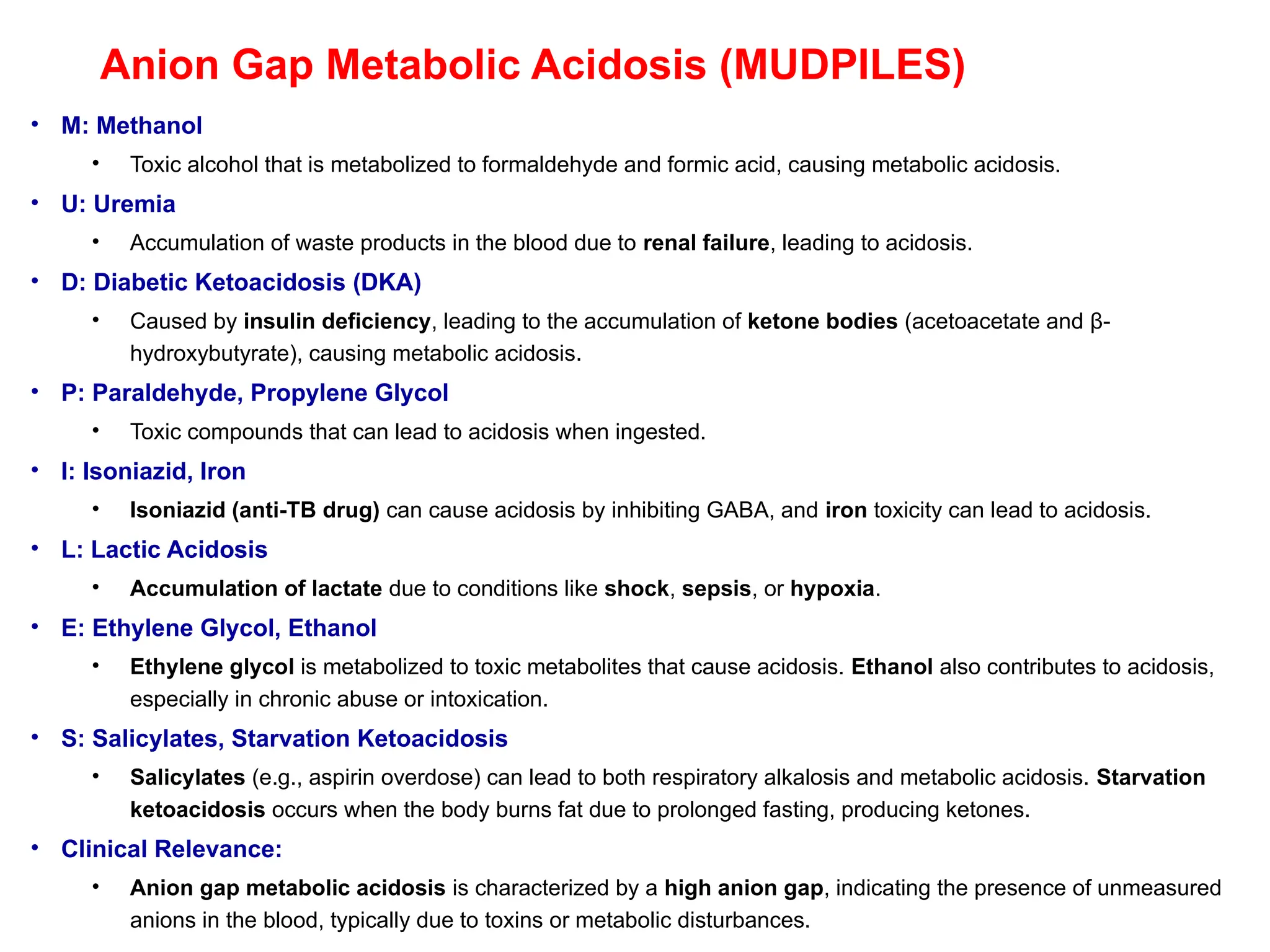
83.
Anion Gap MetabolicAcidosis (MUDPILES)
• M: Methanol
• Toxic alcohol that is metabolized to formaldehyde and formic acid, causing metabolic acidosis.
• U: Uremia
• Accumulation of waste products in the blood due to renal failure, leading to acidosis.
• D: Diabetic Ketoacidosis (DKA)
• Caused by insulin deficiency, leading to the accumulation of ketone bodies (acetoacetate and β-
hydroxybutyrate), causing metabolic acidosis.
• P: Paraldehyde, Propylene Glycol
• Toxic compounds that can lead to acidosis when ingested.
• I: Isoniazid, Iron
• Isoniazid (anti-TB drug) can cause acidosis by inhibiting GABA, and iron toxicity can lead to acidosis.
• L: Lactic Acidosis
• Accumulation of lactate due to conditions like shock, sepsis, or hypoxia.
• E: Ethylene Glycol, Ethanol
• Ethylene glycol is metabolized to toxic metabolites that cause acidosis. Ethanol also contributes to acidosis,
especially in chronic abuse or intoxication.
• S: Salicylates, Starvation Ketoacidosis
• Salicylates (e.g., aspirin overdose) can lead to both respiratory alkalosis and metabolic acidosis. Starvation
ketoacidosis occurs when the body burns fat due to prolonged fasting, producing ketones.
• Clinical Relevance:
• Anion gap metabolic acidosis is characterized by a high anion gap, indicating the presence of unmeasured
anions in the blood, typically due to toxins or metabolic disturbances.
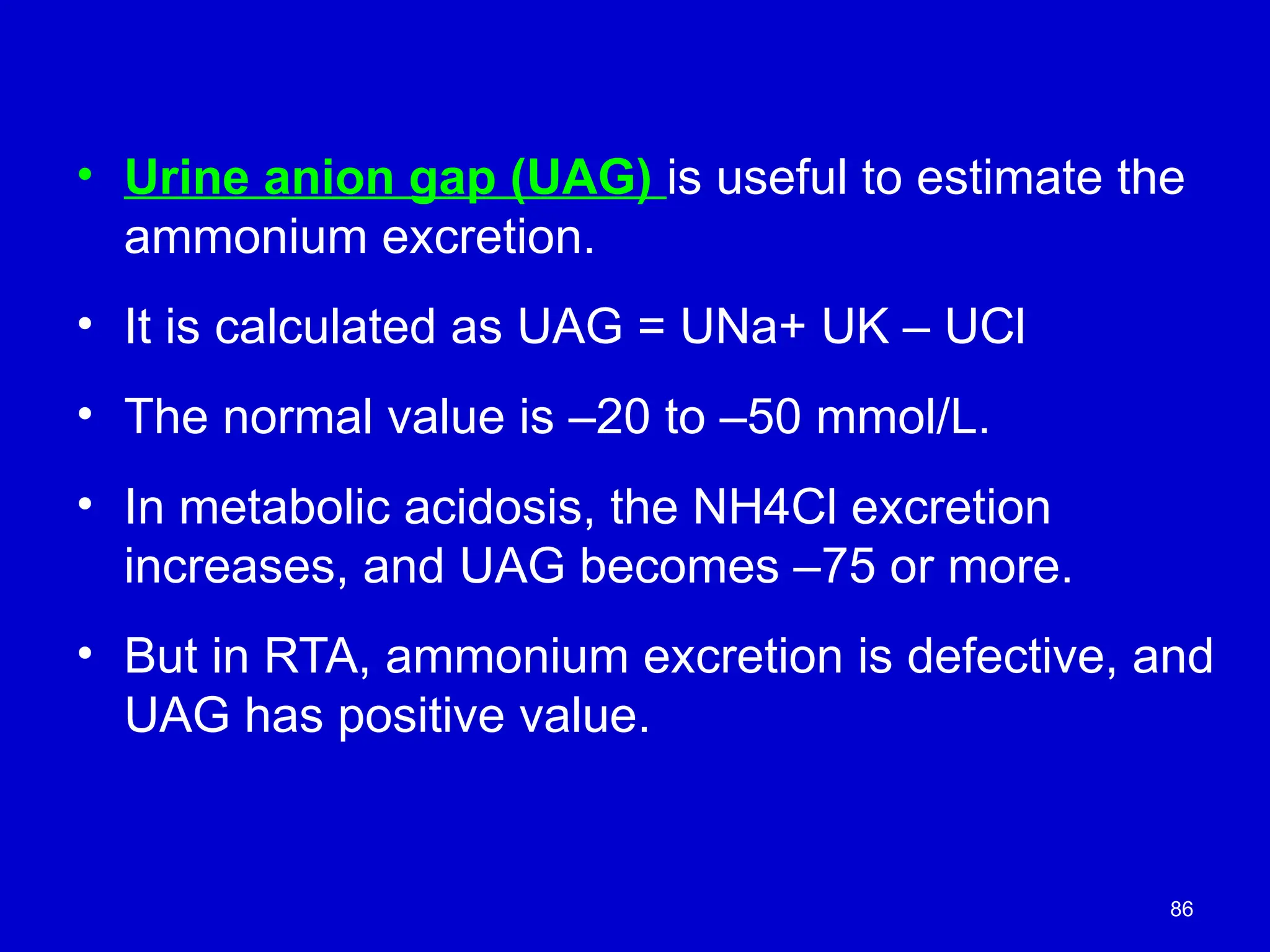
86
• Urine aniongap (UAG) is useful to estimate the
ammonium excretion.
• It is calculated as UAG = UNa+ UK – UCl
• The normal value is –20 to –50 mmol/L.
• In metabolic acidosis, the NH4Cl excretion
increases, and UAG becomes –75 or more.
• But in RTA, ammonium excretion is defective, and
UAG has positive value.
87.
87
The normalosmolal gap is <10 mOsm.
A high osmolal gap (> 25) implies the presence of
unmeasured osmoles such as alcohol, methanol, ethylene
glycol, etc.
Acute poisoning should be considered in patients with a raised
anion gap metabolic acidosis and an increased plasma
osmolal gap.
Poisoning with methanol and ethylene glycol should be
considered.
They are metabolized to formic acid and oxalic acids
correspondingly.
Methanol will produce blindness.
Ethylene glycol will lead to oxalate crystalluria and renal
failure.
88.
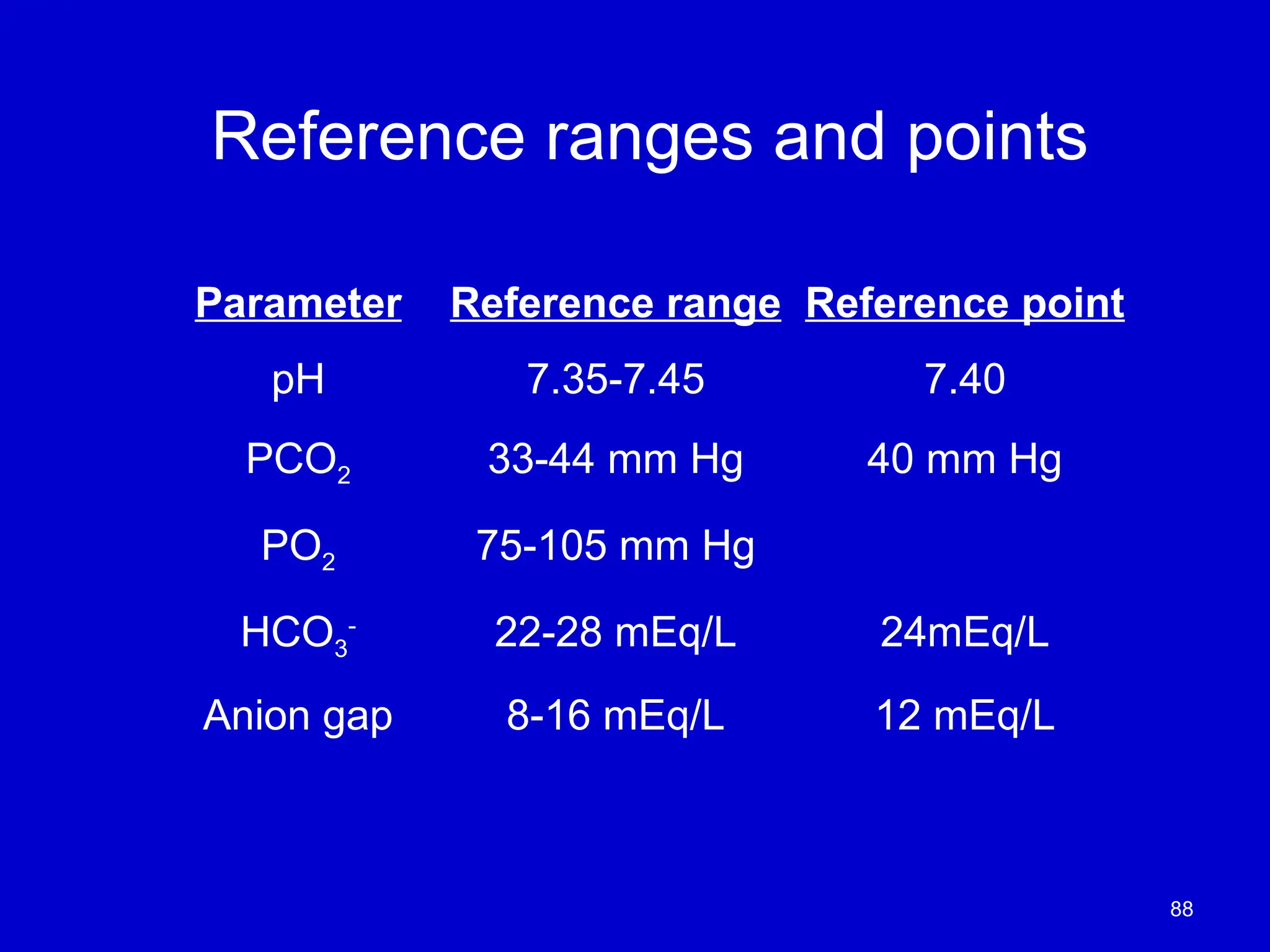
Reference ranges andpoints
Parameter Reference range Reference point
pH 7.35-7.45 7.40
PCO2 33-44 mm Hg 40 mm Hg
PO2 75-105 mm Hg
HCO3
-
22-28 mEq/L 24mEq/L
Anion gap 8-16 mEq/L 12 mEq/L
88
89.
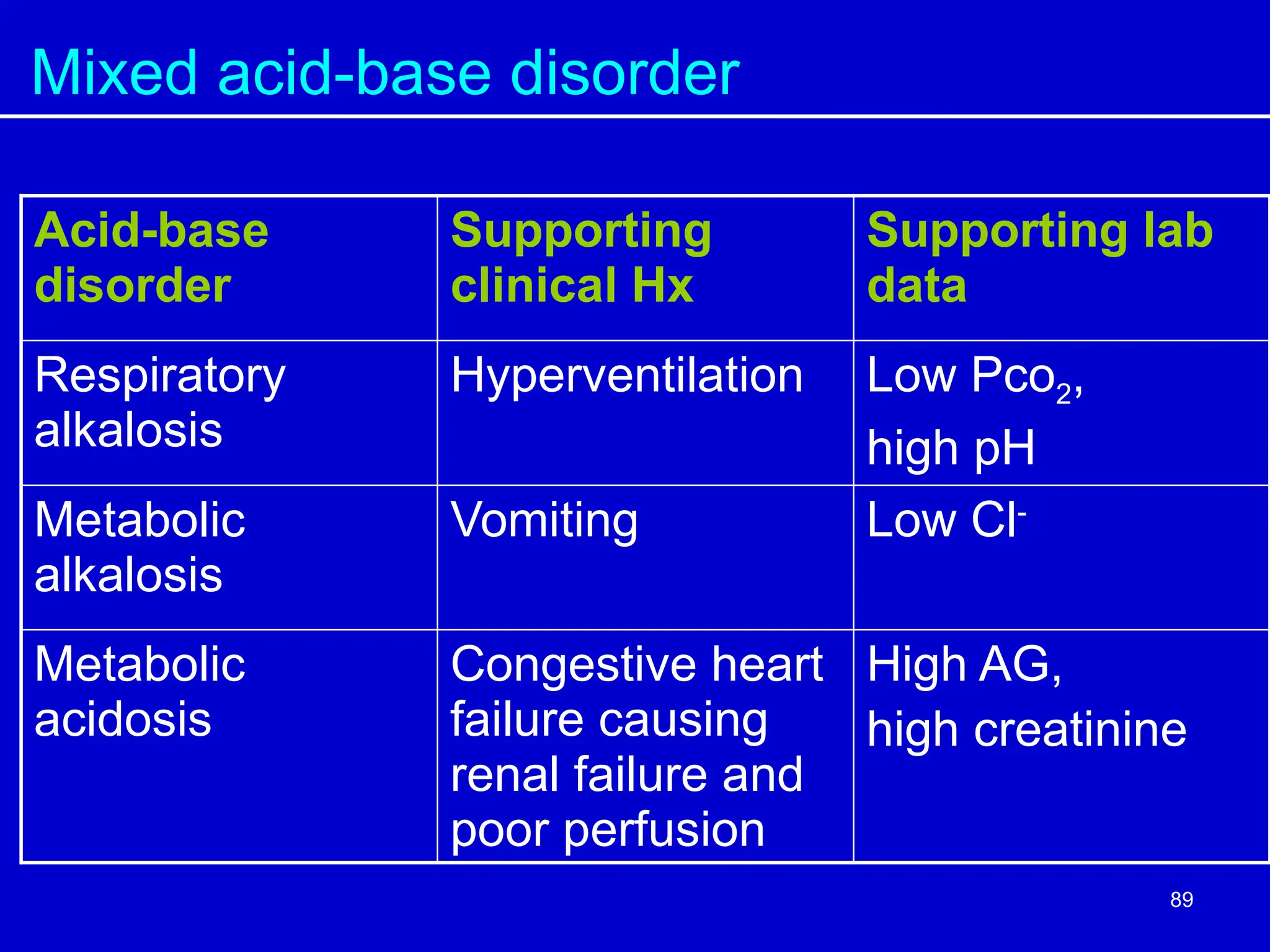
Mixed acid-base disorder
Acid-base
disorder
Supporting
clinicalHx
Supporting lab
data
Respiratory
alkalosis
Hyperventilation Low Pco2,
high pH
Metabolic
alkalosis
Vomiting Low Cl-
Metabolic
acidosis
Congestive heart
failure causing
renal failure and
poor perfusion
High AG,
high creatinine
89
90.
Evaluating the Acid-BaseStatus
• Clinical history
• Electrolyte results (Na+
, K+
, Cl-
, etc)
• Blood gas results (pH, Pco2, HCO3
-
, Po2)
90
91.
Summary: Acid-Base Balanceand Disorders
• Vital Importance of Hydrogen Ion Concentration:
• Maintaining hydrogen ion concentration within a narrow range is crucial for cell survival.
• Regulation of Acid-Base Balance:
• The lungs and kidneys work together to regulate acid-base balance.
• Erythrocytes (red blood cells) play a key role in carbon dioxide transport in the blood.
• Buffers in Blood and Cells:
• Main buffers in blood: Hemoglobin and bicarbonate.
• Main buffers in cells: Proteins and phosphate.
• The bicarbonate buffer system communicates with atmospheric air, maintaining
homeostasis.
• Acid-Base Disorders:
• Two primary acid-base disorders: Acidosis and Alkalosis.
• Disorders can be classified as metabolic or respiratory.
• First-Line Investigations:
• pH, pCO₂, bicarbonate, and pO₂ are essential for diagnosing acid-base disorders, often
required in emergency situations.
#88 PAO2=FIO2(Patm-47)-(PaCO2)/0.8
Anion gap = [Na+] + [UC] – [Cl-] – [HCO3-] – [UA] where UC are K+, Ca2+, and Mg2+ ([UC] = 11 mEq/L) and UA are PO43-, SO42-, proteins and organic acids ([UA] = 20-24 mEq/L).
Osmolar gap = Osmolalitymeasured – 2]Na+] –[Glucose] – [Urea] Osmolarity and osmolality are not the same, but close.
Base deficit: ∆⇑anion gap = ∆⇓HCO3-
Delta gap: (AGpatient – AGnormal) – (HCO3-patient – HCO3-normal) Delta ratio: (AGpatient – AGnormal)/(HCO3-patient – HCO3-normal)
![2
pH
• The concentration of hydrogen ions
determines the acidity of the solution, which
is expressed in terms of pH.
• [H+
] can be expressed as pH
• pH is negative log of [H+
]](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-2-2048.jpg)
![Hydrogen ion concentration
• Blood [H+
] is maintained within tight limits
– Reference values 35-45 nmol/L
– Values > 120 nmol/L or < 20 nmol/L are incompatible
with life
3](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-3-2048.jpg)
![The pH Scale
Understanding the Ion Product of Water
and the pH Scale
•Ion Product of Water (K )
ᴡ :
• K = [H ][OH ]
ᴡ ⁺ ⁻
• Basis for defining the pH scale
•Definition of pH:
• pH = –log[H ]
⁺
• Measures the concentration of
hydrogen ions in a solution
•Neutral Solutions:
• [H ] = [OH ]
⁺ ⁻
• pH = 7.0
•Acidic Solutions:
• [H ] > [OH ]
⁺ ⁻
• pH < 7.0
•Basic Solutions:
• [H ] < [OH ]
⁺ ⁻
• pH > 7.0](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-5-2048.jpg)
![6
Water itself is neutral, neither acidic
nor basic.
The pH of pure water is 7
A pH of 7 is termed neutral because [H+] and [OH−]
are equal](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-6-2048.jpg)
![Acid-Base Disorders
• Acidosis
– [H+
] above normal (low pH)
– ratio [HCO3
-
/Pco2] < 20
• Alkalosis
– [H+
] below normal (high pH)
– ratio [HCO3
-
/Pco2] > 20
pH = pK + log[HCO3
-
/Pco2]
10
[HCO3 –
] = 24.0 mM, and [CO2]= 1.20 mM.
Normal values for these are pH = 7.40,](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-10-2048.jpg)
![Metabolism
Cell
CO2
H+
Plasma
Plasma
(15,000mmol/d)
(40-80mmol/d)
Lungs
Kidney
Production & Excretion of H+
ions
[H+
] = 35 – 45 nmol/L
13](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-13-2048.jpg)

![Primary Alteration in CO2
Respiratory Acidosis (10
CO2 excess)
CO2 + H2O ↔ H2CO3↔ H+
+ HCO3- =pH
Blood
Causes
Hypoventilation (CO2 retention)
- airway obstruction
- depression of respiratory center
- neuromuscular disease
pH = pK + log[HCO3
-
]
[Pco2]
Ratio < 20
62](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-62-2048.jpg)
![Compensation in Respiratory Acidosis
• slowly, kidney
– increases H+
excretion
– increases HCO3
-
regeneration
• Net effect: increase of plasma [HCO3
-
]
[HCO3
-
]
[Pco2]
pH moves up towards normal.
63](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-63-2048.jpg)
![Primary Alteration in CO2
Respiratory Alkalosis (10
CO2 deficit)
CO2 + H2O ↔ H2CO3↔ H+
+ HCO3- =pH
Causes
Hyperventilation
- hypoxemia/hypoxia
- increased respiratory center
- pulmonary disease
- metabolic acidosis
pH = pK + log[HCO3
-
]
[Pco2]
Ratio > 20
64](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-64-2048.jpg)
![Compensation in Respiratory Alkalosis
• Slowly, several days
– renal H+
excretion decreased
• Net effect is to increase renal HCO3
-
loss
[HCO3
-
]
[Pco2]
pH moves down towards normal.
65](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-65-2048.jpg)
![Primary Alteration in Bicarbonate
Non-respiratory (metabolic) Acidosis (10
HCO3
-
deficiency)
CO2 + H2O ↔ H2CO3↔ H+
+ HCO3-
Causes
• H+
overload - ketoacidosis (DKA also alcoholic)
- lactic acidosis
- poisoning (salicylate, ethanol)
• Defects of H+ excretion
- CRF
- RTA (H+
pump defect)
• Bicarbonate loss
- diarrhoea
- pancreatic drainage
pH = pK + log [ HCO3
-
]
[Pco2]
Ratio < 20
66](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-66-2048.jpg)
![Compensation in Metabolic Acidosis
• Respiratory center is stimulated causing
increased loss of CO2
• Kidney
– increases the excretion of acid
– increases reabsorption of [HCO3
-
]
[HCO3
-
]
[Pco2]
pH moves up towards normal. 67](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-67-2048.jpg)
![Primary Alteration in Bicarbonate
Non-respiratory (metabolic) Alkalosis (10
HCO3
-
excess)
CO2 + H2O ↔ H2CO3↔ H+
+ HCO3-
Causes
• Loss of H+
- vomiting
- gastric aspiration
- renal - K+
depletion
- mineralocorticoid excess
- diuretic therapy
• Overload with alkali (rare)
pH = pK + log [ HCO3
-
]
[Pco2]
Ratio > 20
68](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-68-2048.jpg)
![Compensation in Metabolic Alkalosis
• Effect is to decrease the respiratory center
causing a retention of CO2 -minimal
• Kidney
– forms less ammonia
– renal H+
excretion decreased
– Decreases reabsorption of [HCO3
-
]
[HCO3
-
]
[Pco2]
pH moves down towards normal.
69](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-69-2048.jpg)
![The Four Cardinal Acid Base Disorders
M acidosis
M alkalosis
R acidosis
R alkalosis
Disorder pH pCO2 [HCO3
-
]
70](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-70-2048.jpg)
![Anion Gap
is the difference between the total conc. of
measured cations and that of measured anions
Anion Gap (A-) = ([Na+
] + [K+
]) – ([Cl-
] + [HCO3
-
])
RR: 12 - 20 mmol/l
79](https://image.slidesharecdn.com/3-250625213951-804bf9dc/75/3-A-B-balance-revised-ppt-pptx-on-the-renal-system-79-2048.jpg)






































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)









