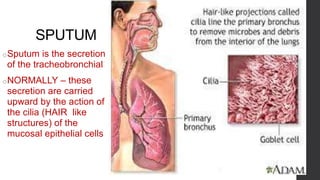
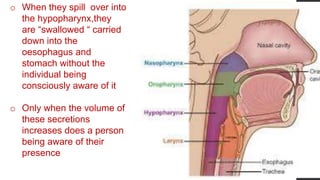
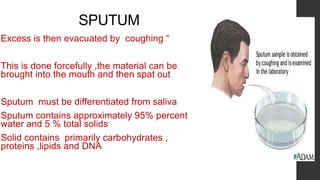
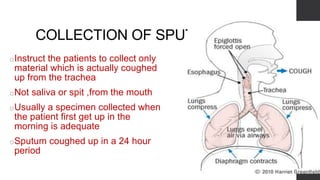
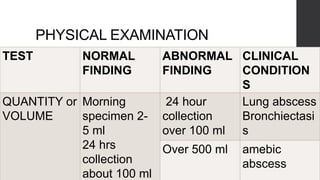
The document discusses examination of sputum. Sputum is normally cleared from the lungs by cilia, but excess collects when coughing. Sputum should be collected in sterile containers and examined while fresh. Physical properties like color, consistency and cell content provide clinical information. Microscopic examination of stained sputum smears allows identification of cells, parasites, fungi and pathogens like tubercle bacilli. Analysis of sputum properties aids diagnosis of lung conditions.