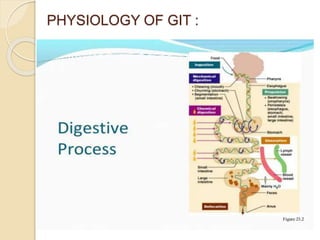
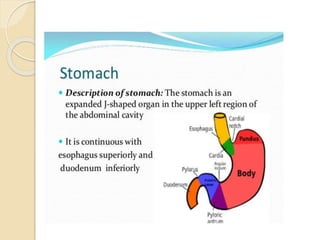
The document discusses the anatomy, histology, physiology, and cytology of the gastrointestinal tract. It provides details on:
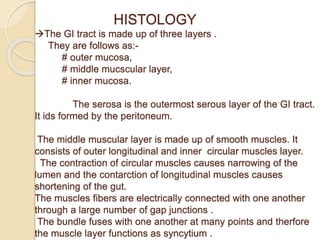
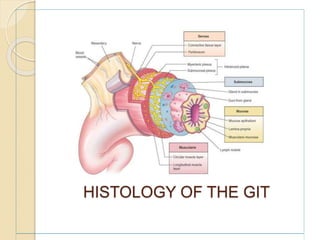
- The layers of the GI tract including the mucosa, muscularis, and serosa.
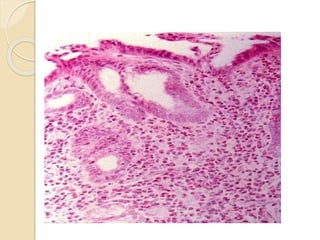
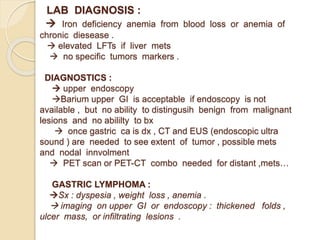
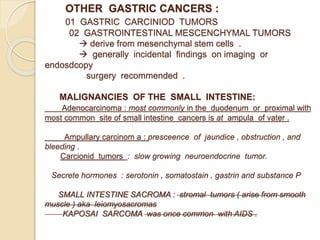
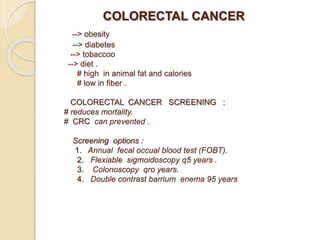
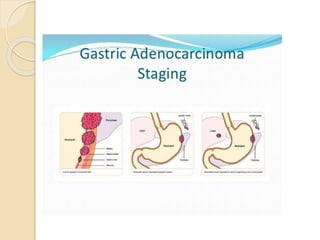
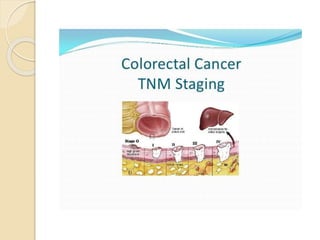
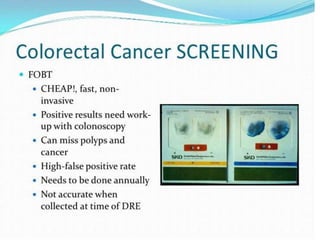
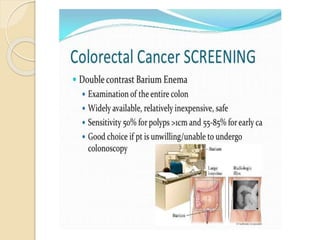
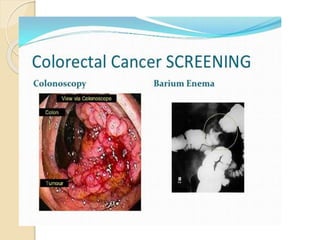
- Common malignant conditions like gastric adenocarcinoma, gastric lymphoma, and colorectal cancer. Risk factors, symptoms, diagnosis and screening are covered.
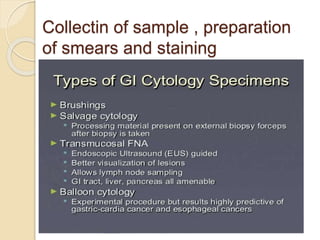
- Non-malignant GI conditions and techniques for sample collection, smear preparation, and staining of GI biopsy specimens.













































![MALIGNANT CANCER OF THE STOMARCH [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/malignantcancerofthestomarchautosaved-250510054659-d24799df-thumbnail.jpg?width=640&height=640&fit=bounds)













































