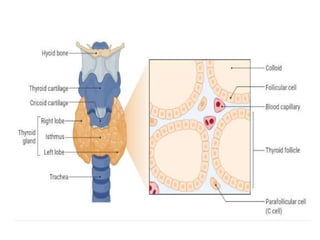
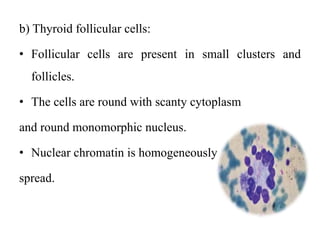
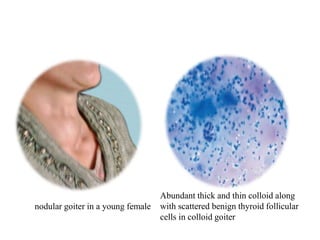
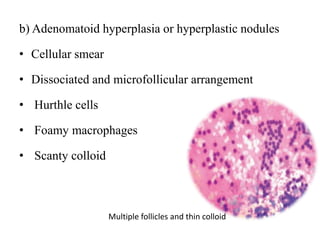
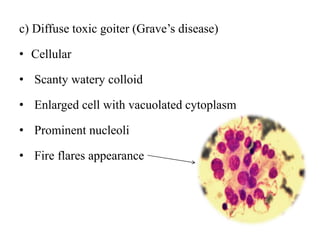
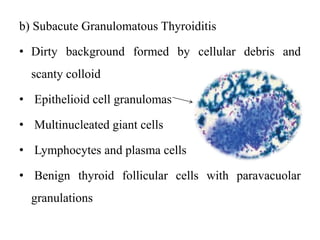
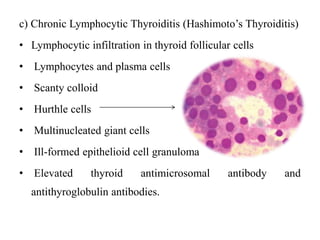
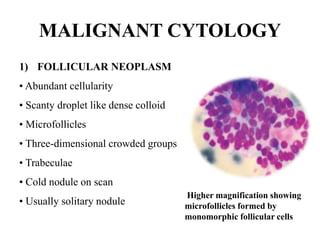
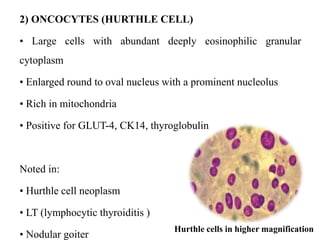
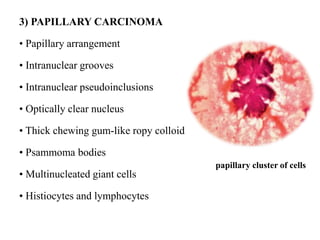
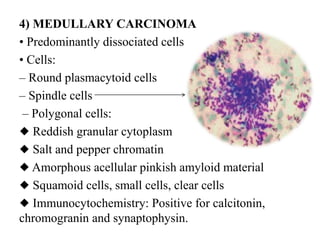
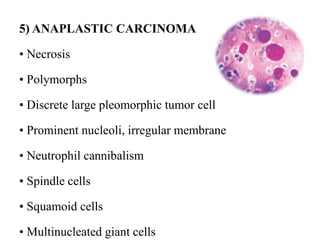
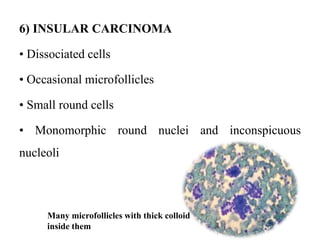
The thyroid gland is located in the neck and is composed of two lobes connected by an isthmus. It contains follicles lined by follicular cells that secrete thyroid hormones. Parafollicular cells secrete calcitonin. Fine needle aspiration cytology is used to evaluate thyroid nodules and can identify normal thyroid tissue, non-malignant conditions like goiter and thyroiditis, and malignant tumors including follicular neoplasms, Hurthle cell neoplasms, papillary carcinoma, medullary carcinoma, anaplastic carcinoma, and insular carcinoma based on cellular appearance and arrangement.