Downloaded 523 times
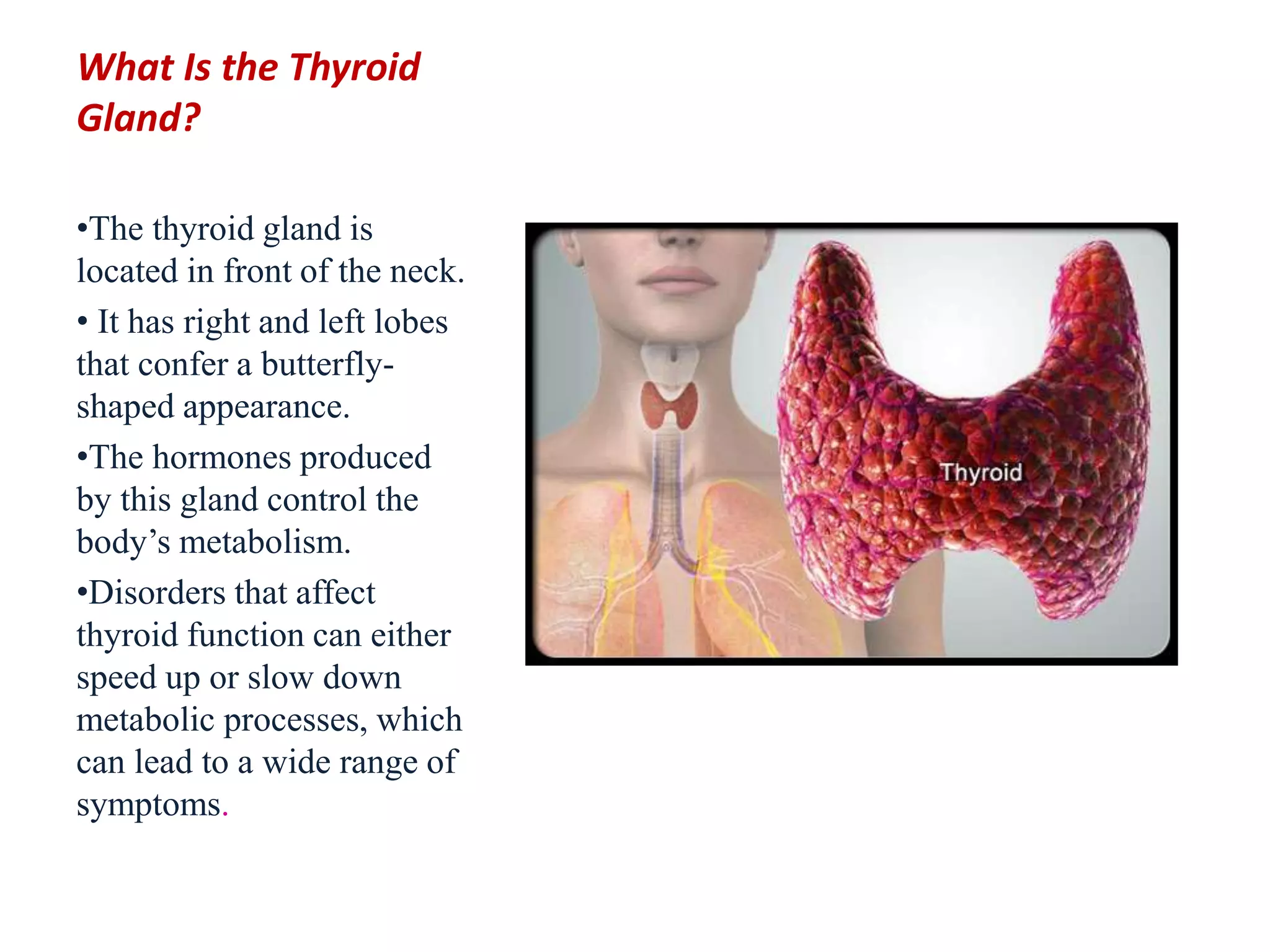
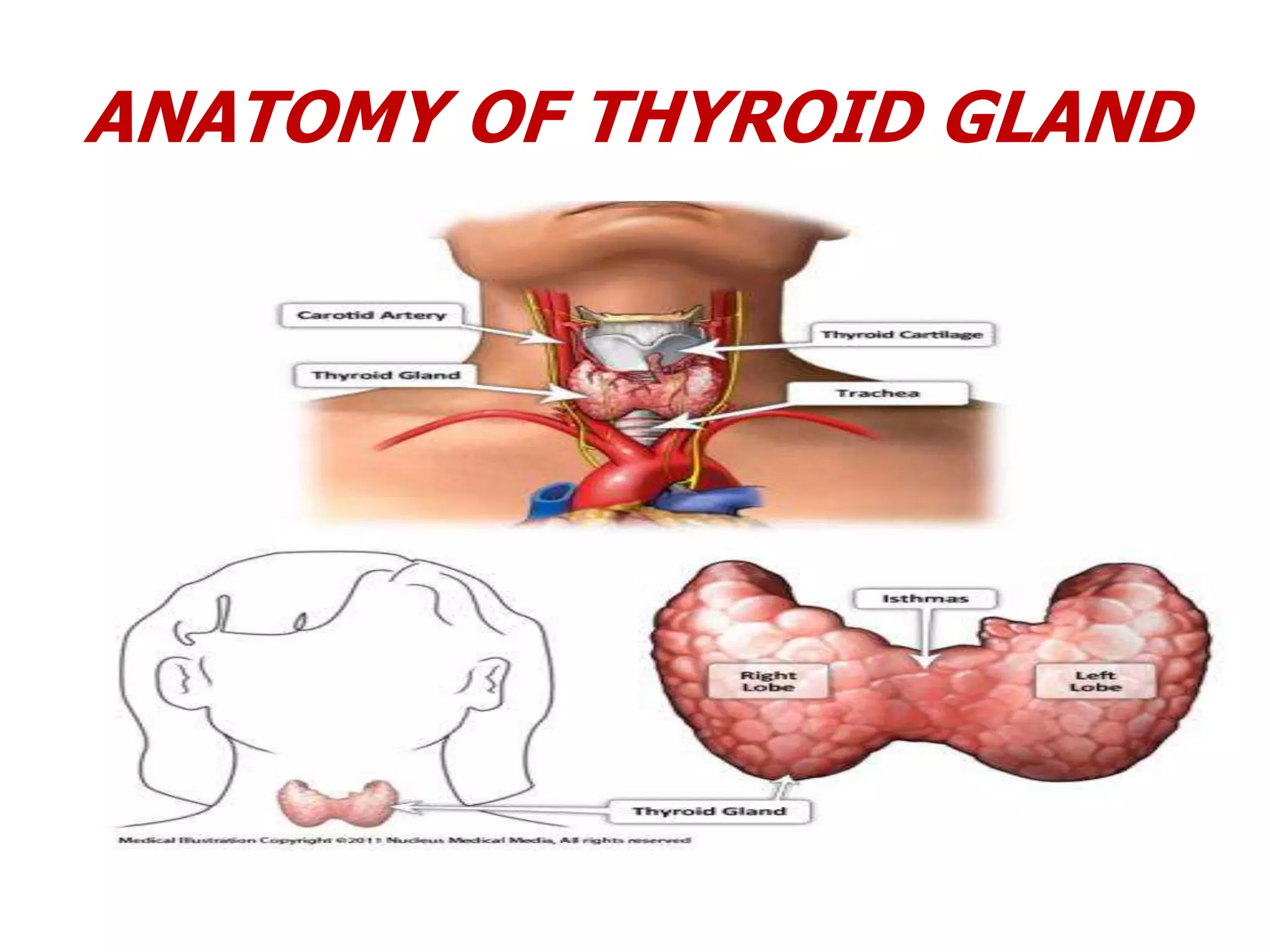
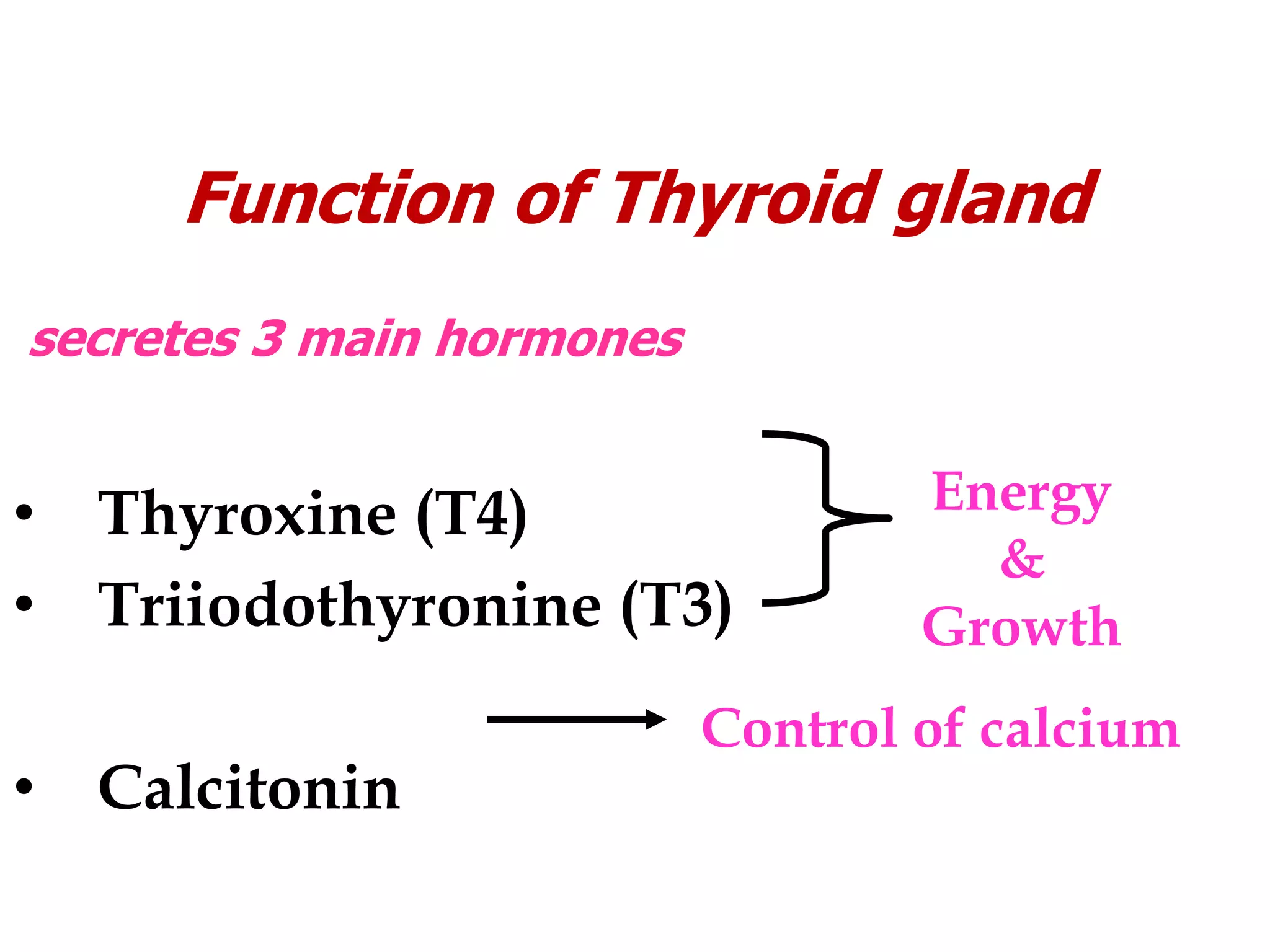
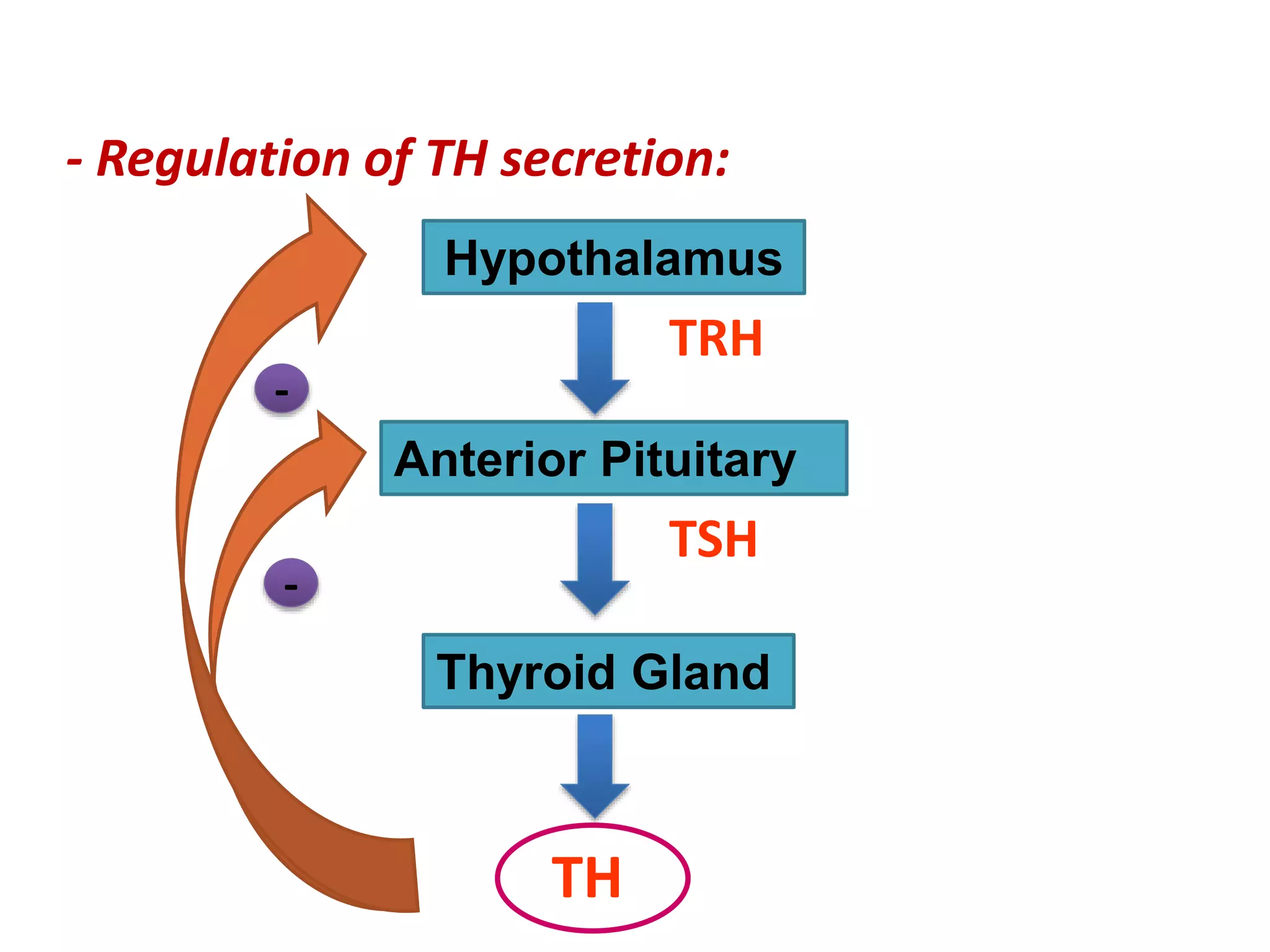
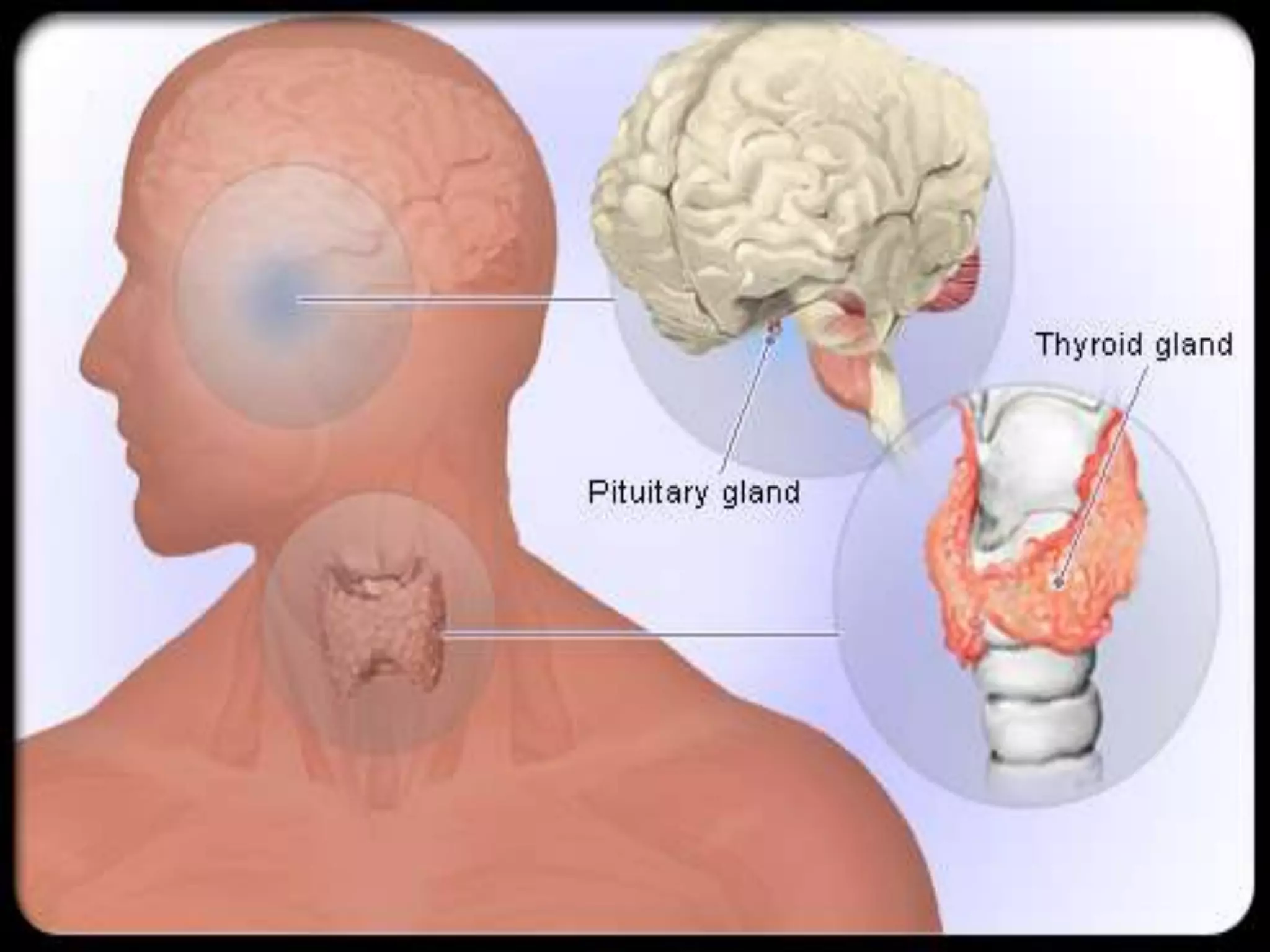
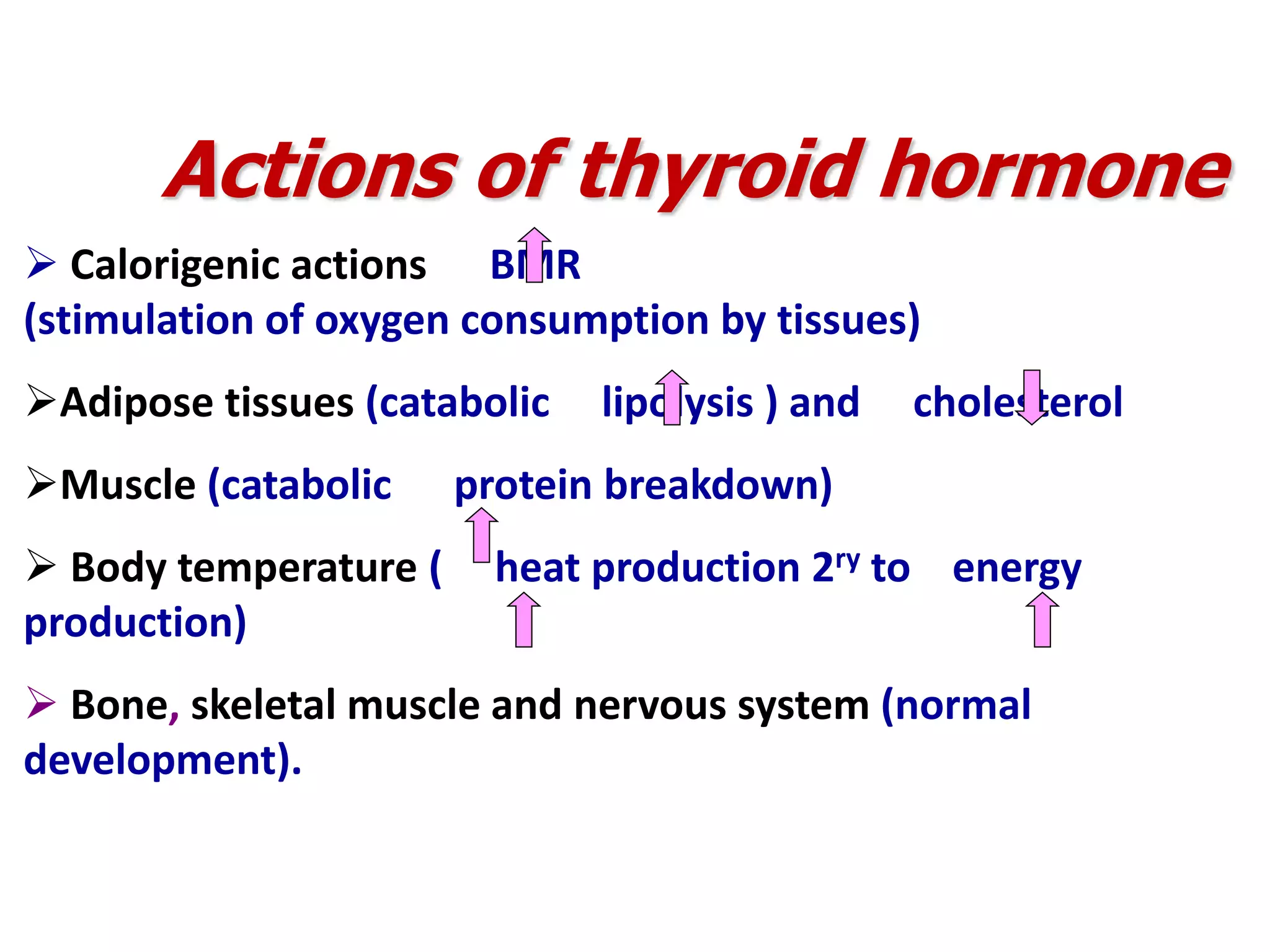
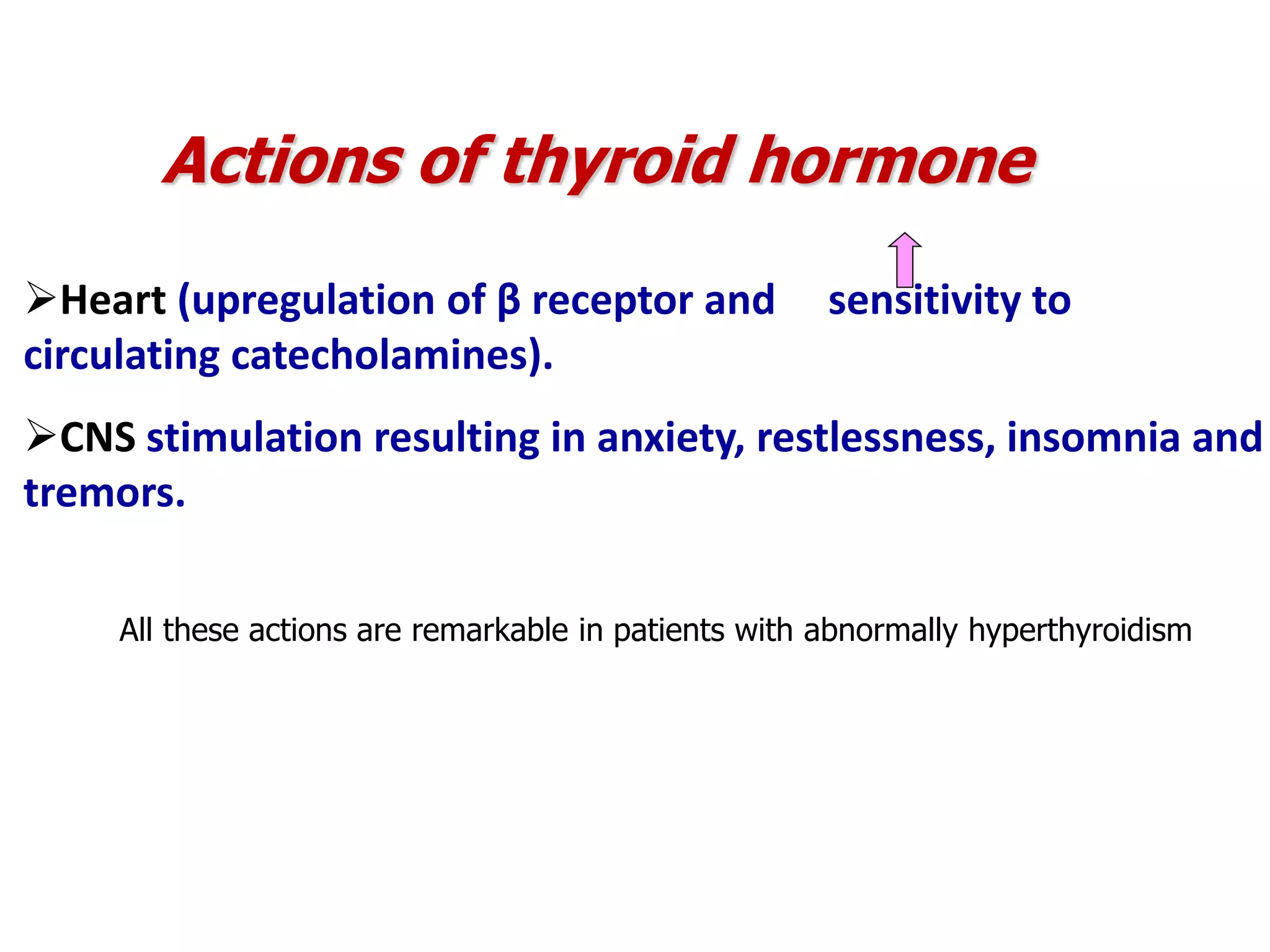
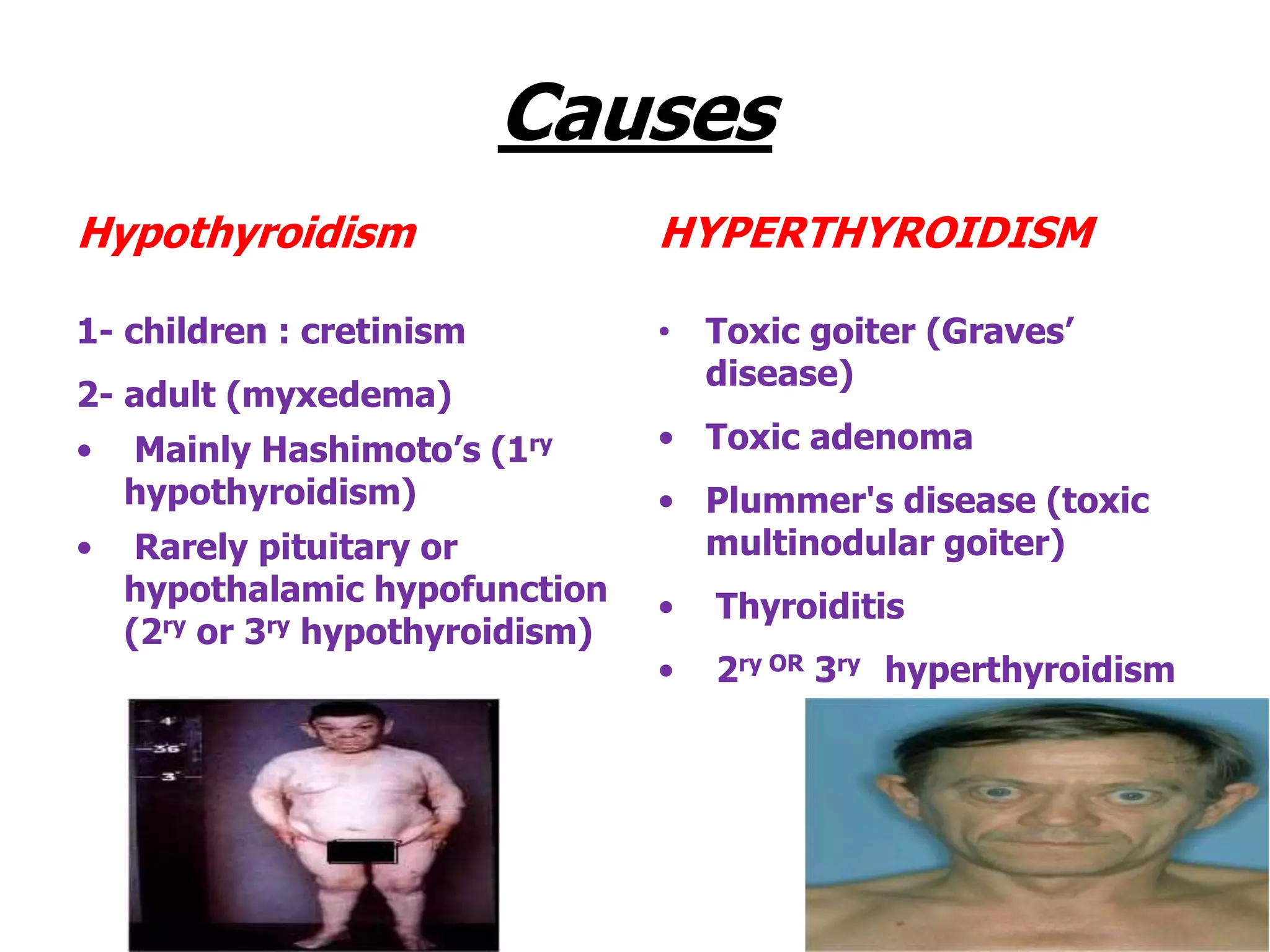
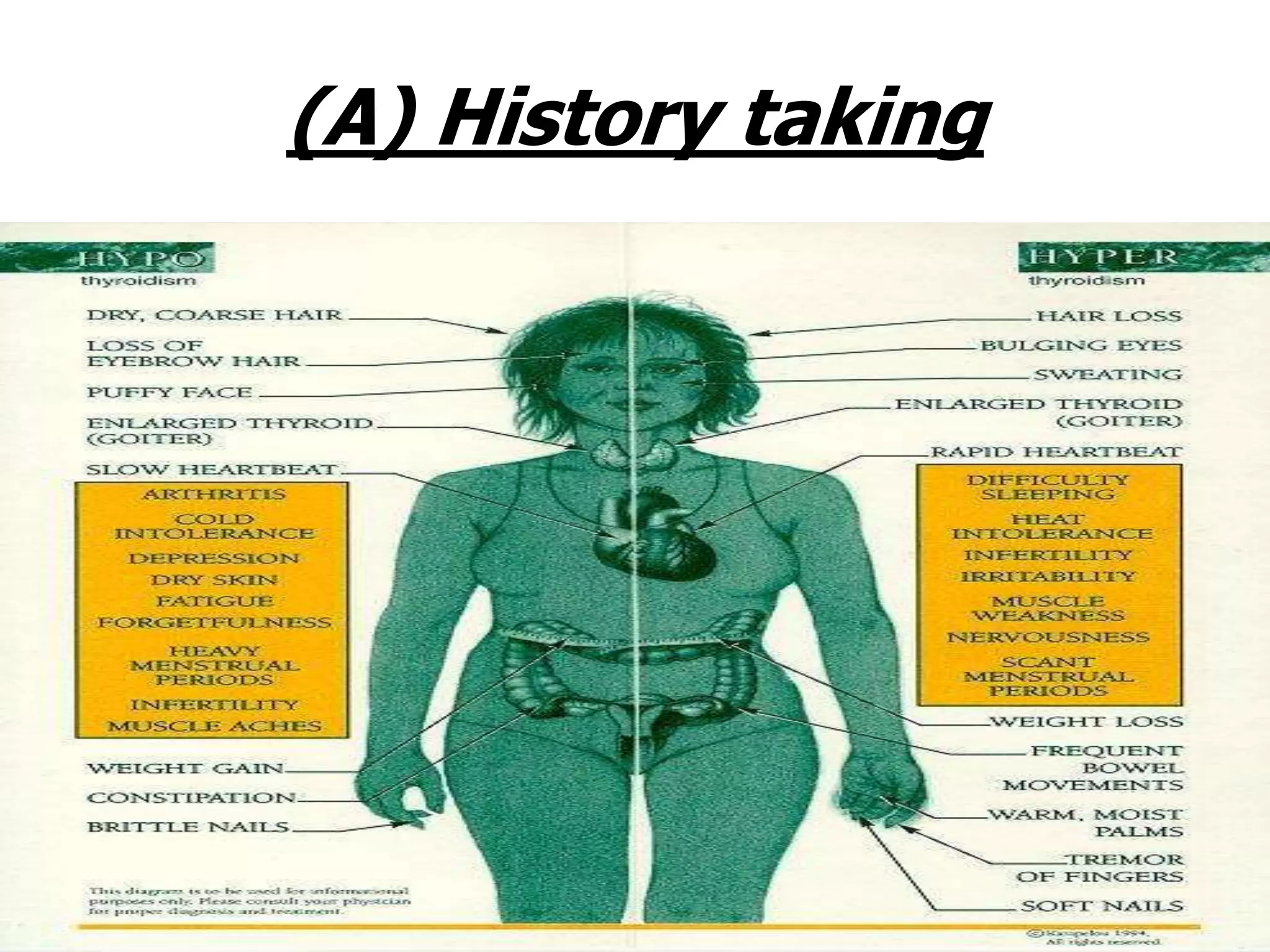
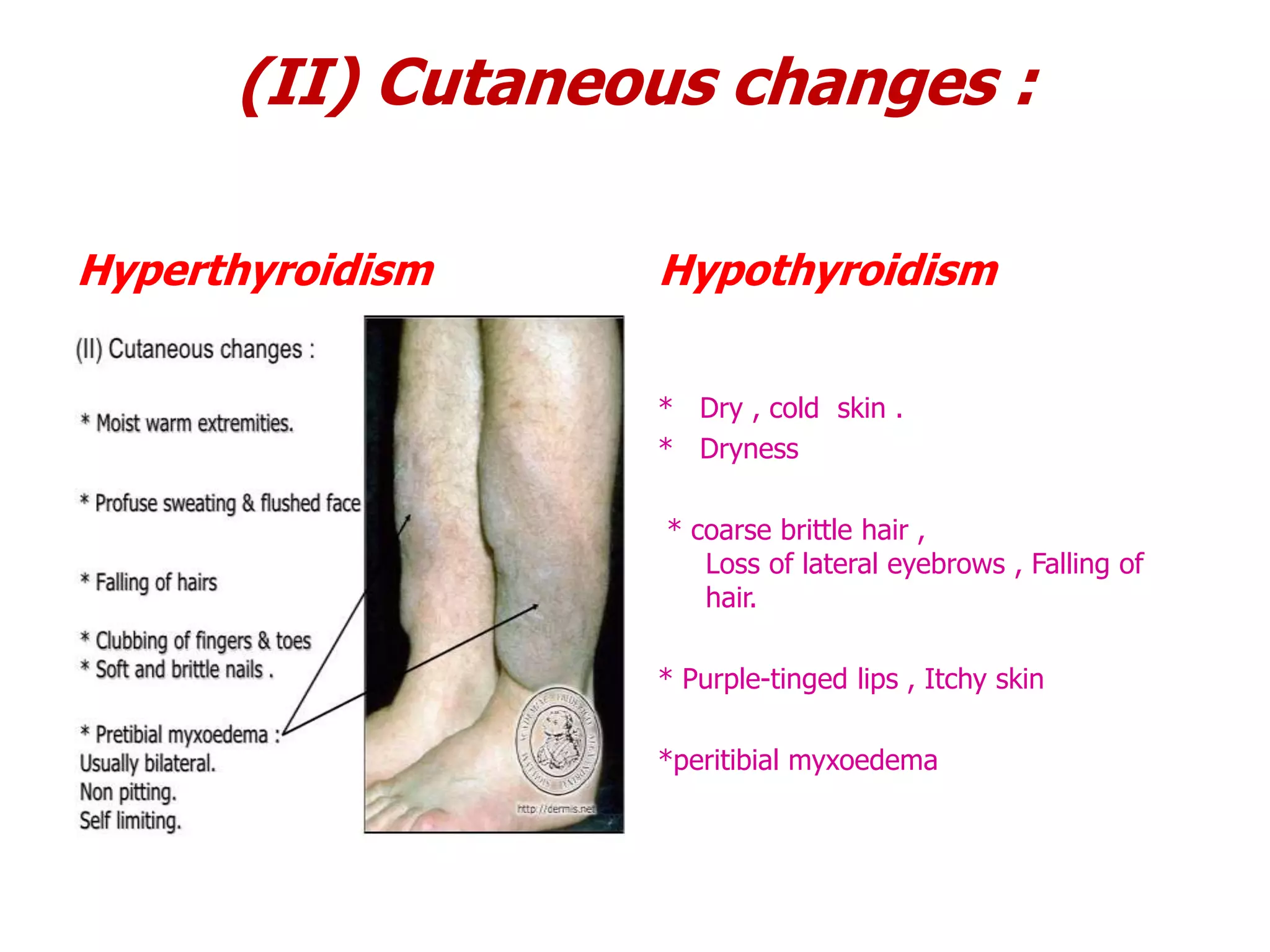
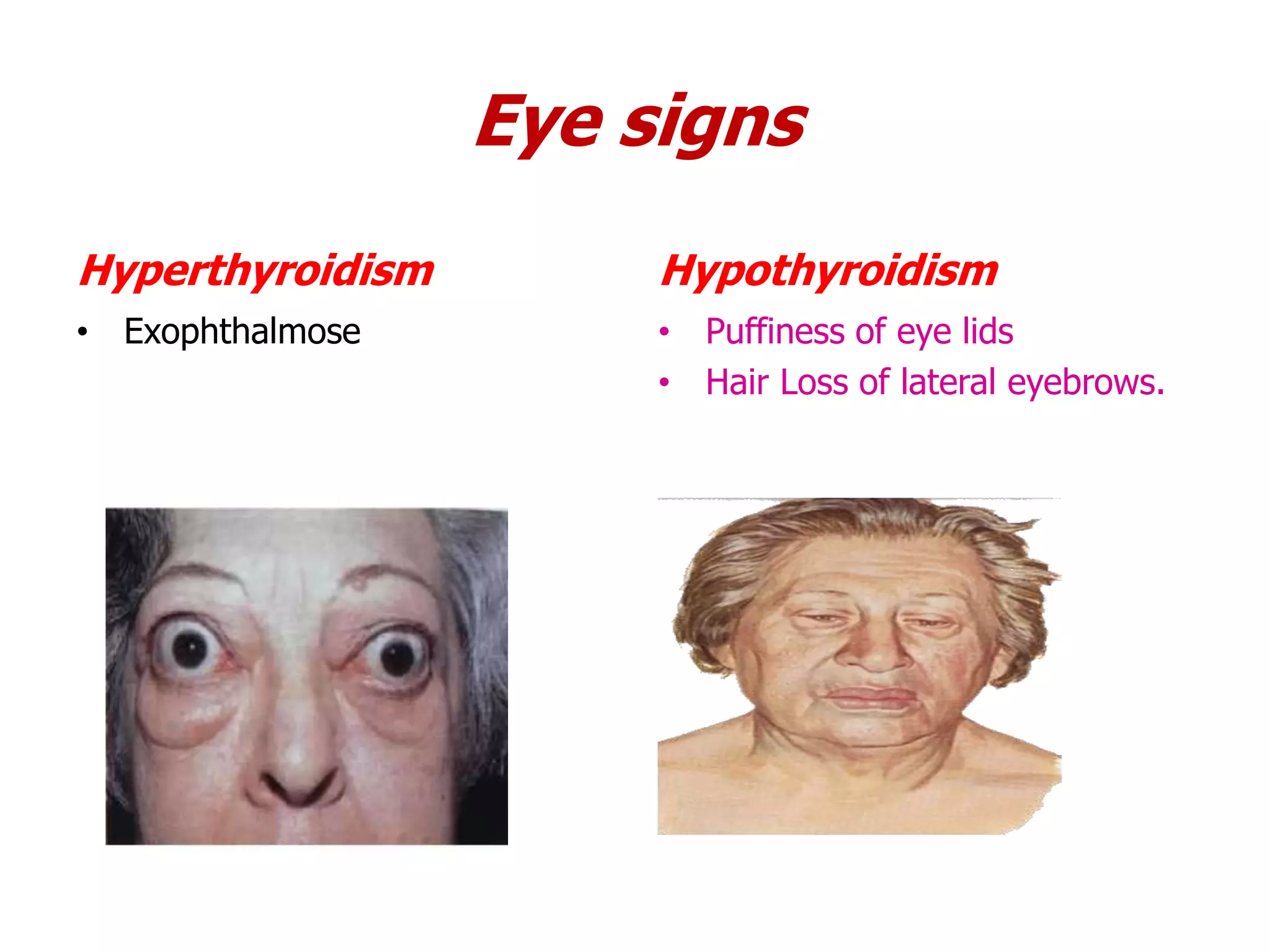
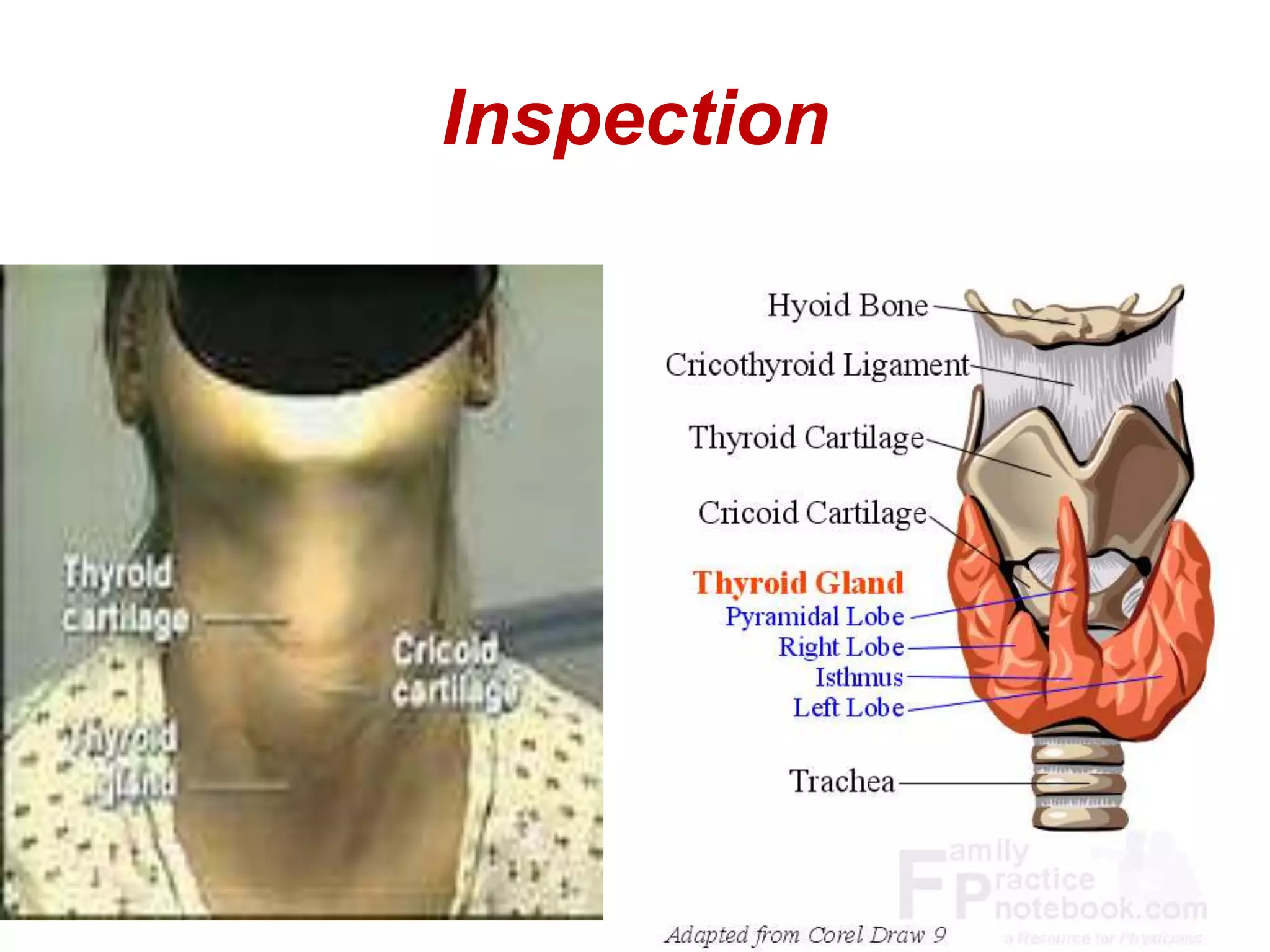

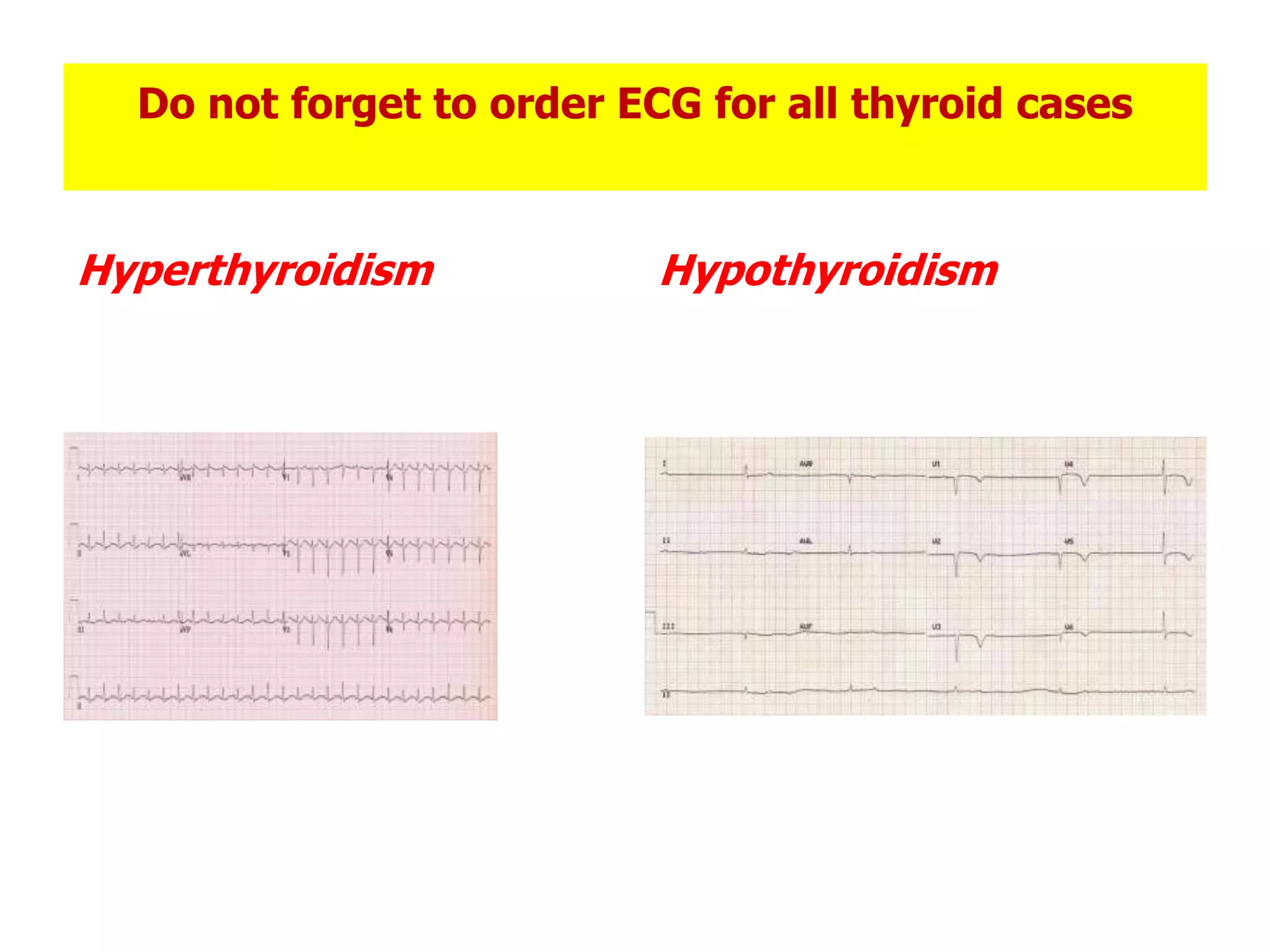
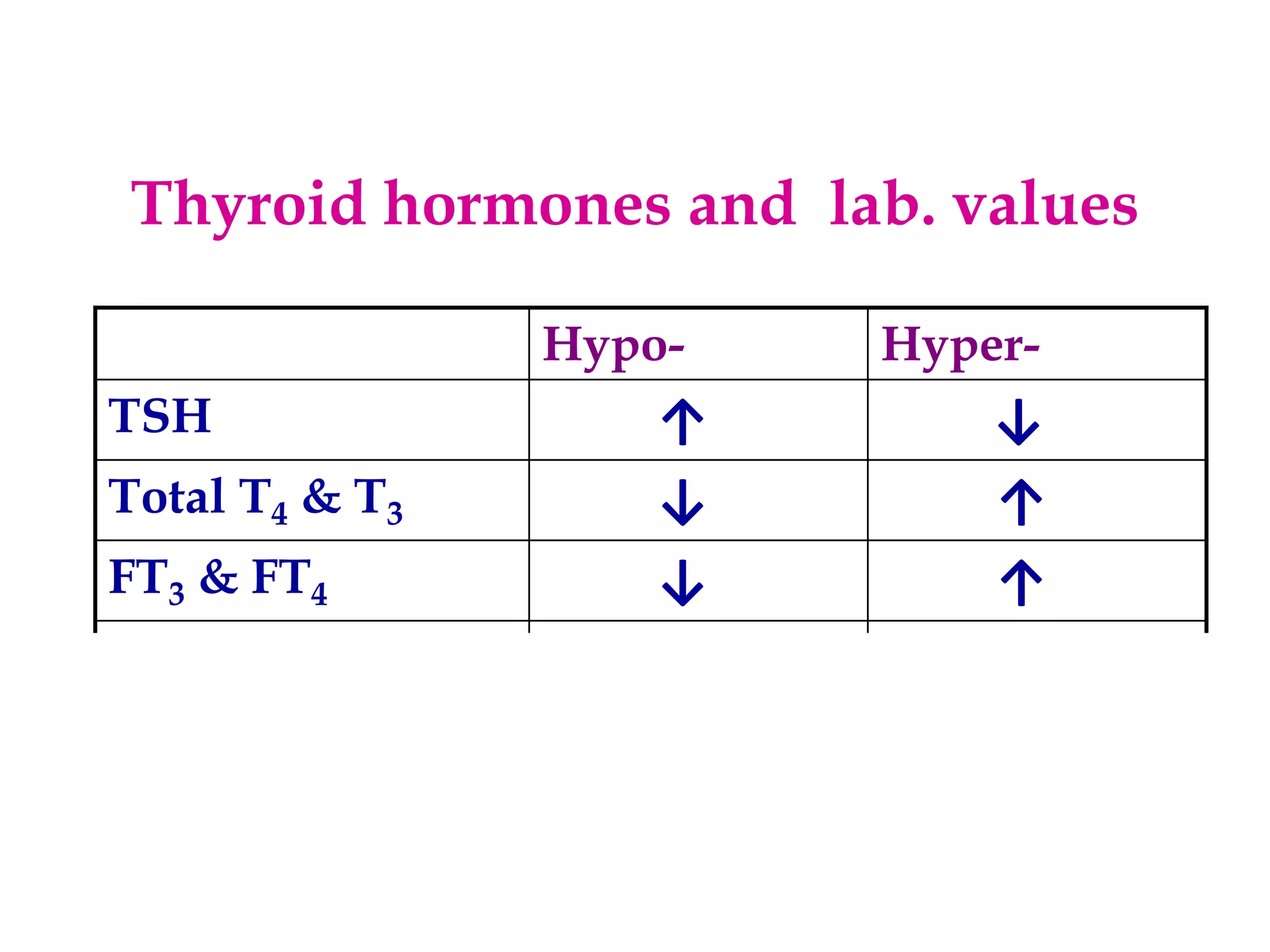
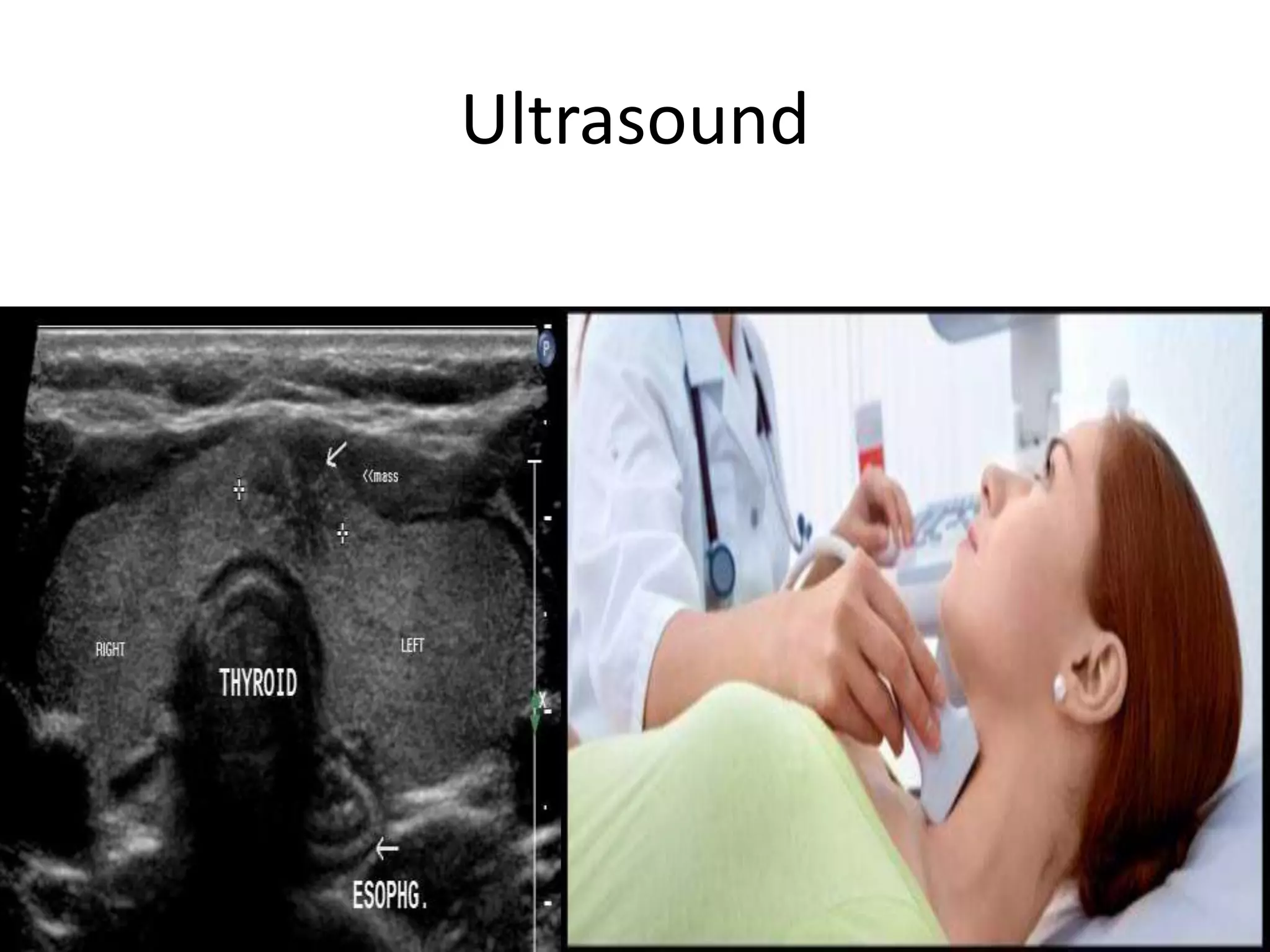
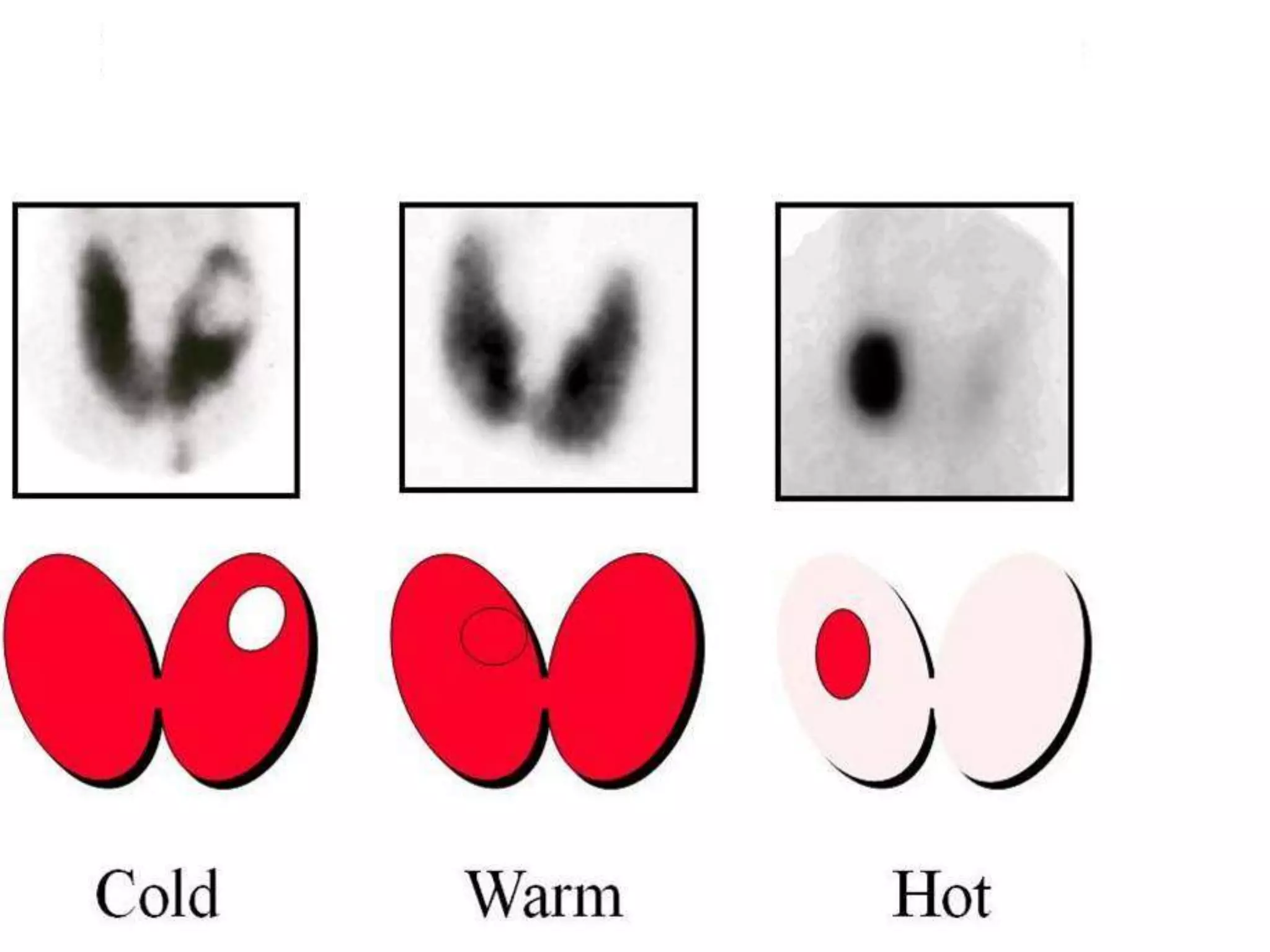

The thyroid gland secretes hormones that regulate metabolism. Disorders can cause hyperthyroidism (overactive thyroid) or hypothyroidism (underactive thyroid). Examination of the thyroid involves inspection for size/shape, palpation for consistency/nodules, and auscultation for bruits. Blood tests measure thyroid hormone levels while ultrasound images the gland. Mild cases may only require monitoring but severe or abnormal cases should be referred to an endocrinologist.





















































![THYROID DISORDERS AND ANAESTHESIA.ppt[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/thyroiddisordersandanaesthesia-240826093351-632c8bba-thumbnail.jpg?width=640&height=640&fit=bounds)







































