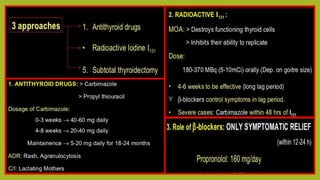
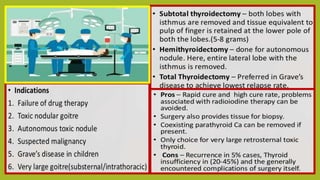
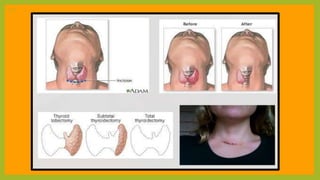
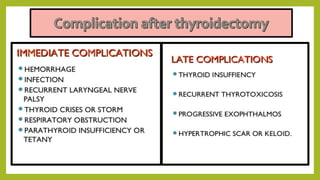
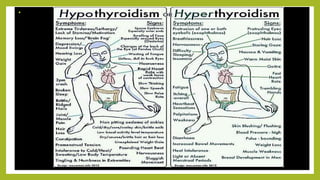
This document provides information on the management of patients with hyperthyroidism and hypothyroidism. It discusses the anatomy and function of the thyroid gland. It describes the different types of thyroid hormones and their regulation. It also covers the etiology, signs and symptoms, diagnosis, and treatment of both hyperthyroidism and hypothyroidism. Nursing care focuses on monitoring for symptoms, managing nutrition and mood, and ensuring patients are euthyroid before surgery to treat hyperthyroidism.









































![THYROID DISORDERS AND ANAESTHESIA.ppt[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/thyroiddisordersandanaesthesia-240826093351-632c8bba-thumbnail.jpg?width=640&height=640&fit=bounds)



































