Downloaded 3,954 times
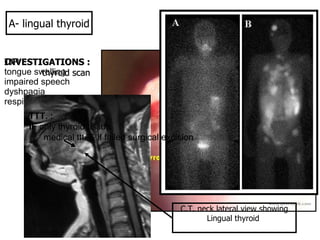

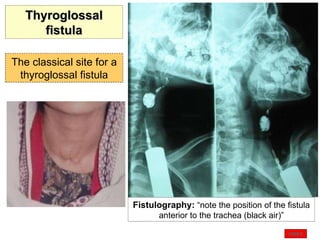

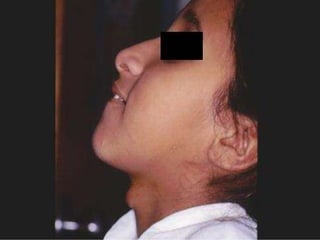

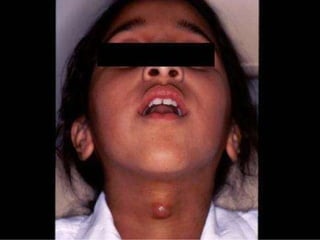
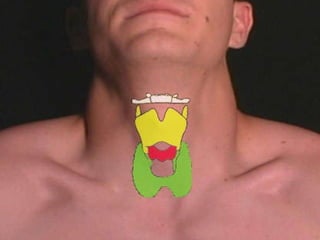
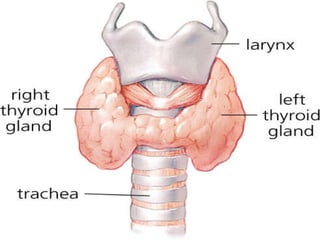





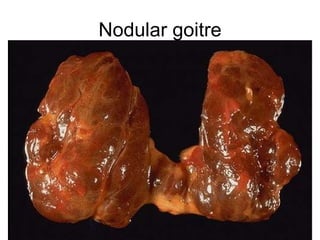











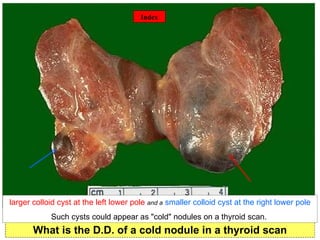


1. Lingual thyroid is a rare condition where the thyroid gland is located at the base of the tongue instead of the normal location in the neck. Investigations like thyroid scan and CT neck can help locate the gland. Treatment involves medical therapy initially and surgery if medical treatment fails. 2. Thyroglossal cysts arise from remnants of the thyroglossal duct during embryonic development of the thyroid gland. Sistrunk operation is the treatment of choice which involves removal of the cyst along with a portion of the hyoid bone and any connecting tract. 3. A cold nodule seen on a thyroid scan could indicate a benign cyst, colloid nodule, or follicular carcinoma of the thyroid


































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


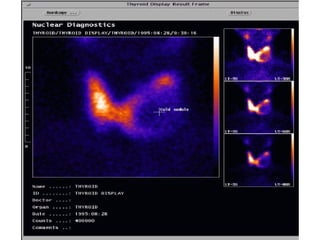
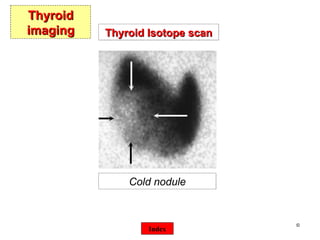
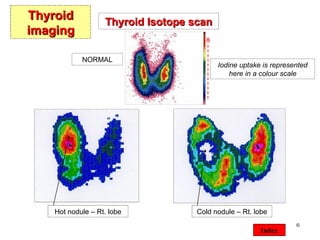
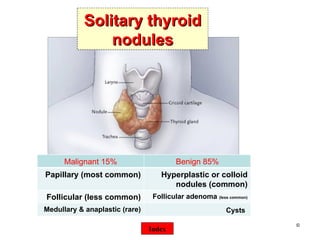
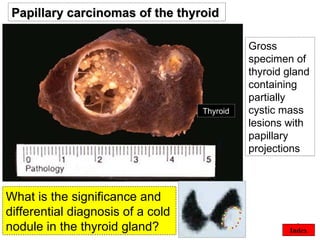
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










