Downloaded 473 times
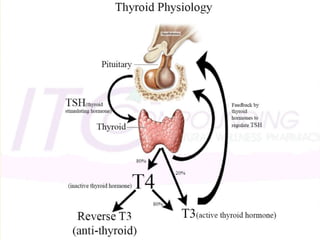
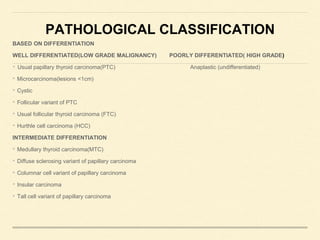

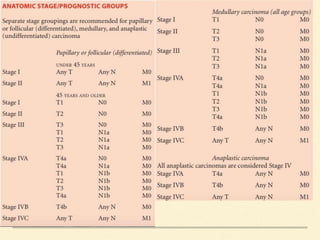


This document discusses the anatomy, physiology, pathology, staging, diagnosis, and treatment of thyroid cancer. Some key points: - The thyroid gland is located in the neck and produces thyroid hormones which regulate metabolism. Thyroid cancers are classified based on their level of differentiation. - Diagnostic evaluation includes laboratory tests, ultrasound of the thyroid, and fine needle aspiration if a nodule is detected. Prognostic factors like histology, stage, and tumor size help determine a patient's risk level. - Surgical treatment typically involves total thyroidectomy. Lymph node dissection may also be performed. Postoperative radioactive iodine remnant ablation is recommended for intermediate- and high-risk










































![Thyroid carcinoma final [part 2]](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidcarcinomafinalpart2-161126043433-thumbnail.jpg?width=640&height=640&fit=bounds)




















![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)









