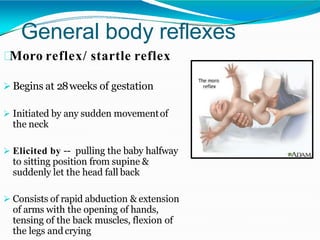
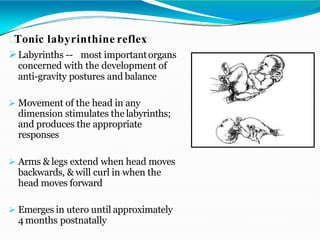
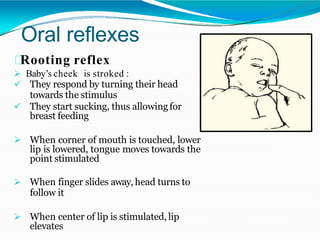
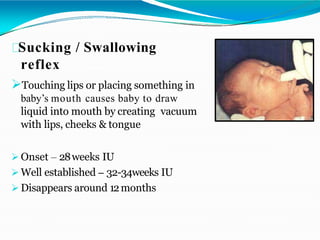
Neonatal reflexes are involuntary responses to stimuli that are present at birth and provide important clues about neurological development. The document describes various reflexes like the moro, rooting, and gag reflex and explains how they are elicited and their significance. Understanding reflex development helps assess normal motor skills progression and identify potential abnormalities.