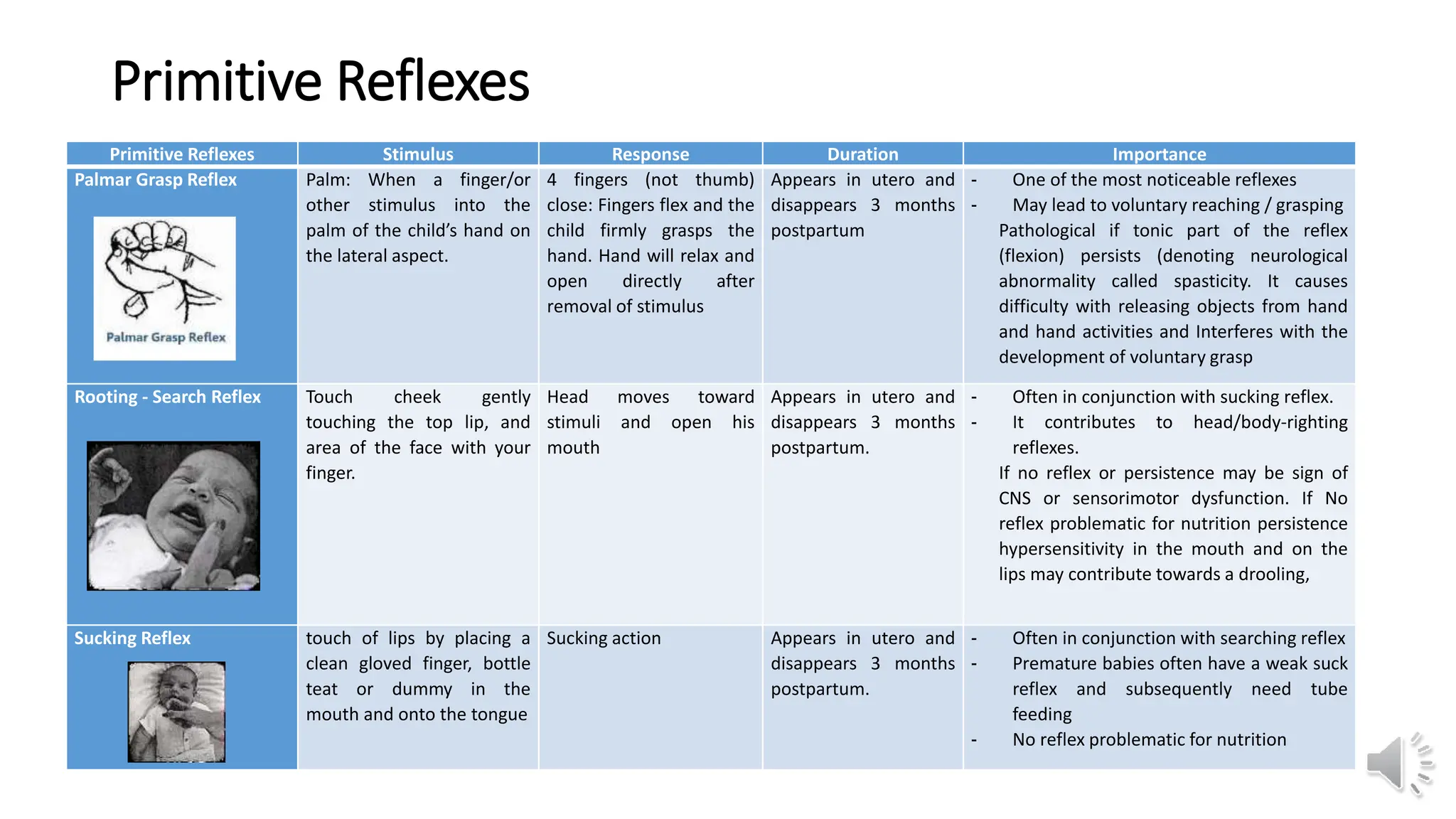
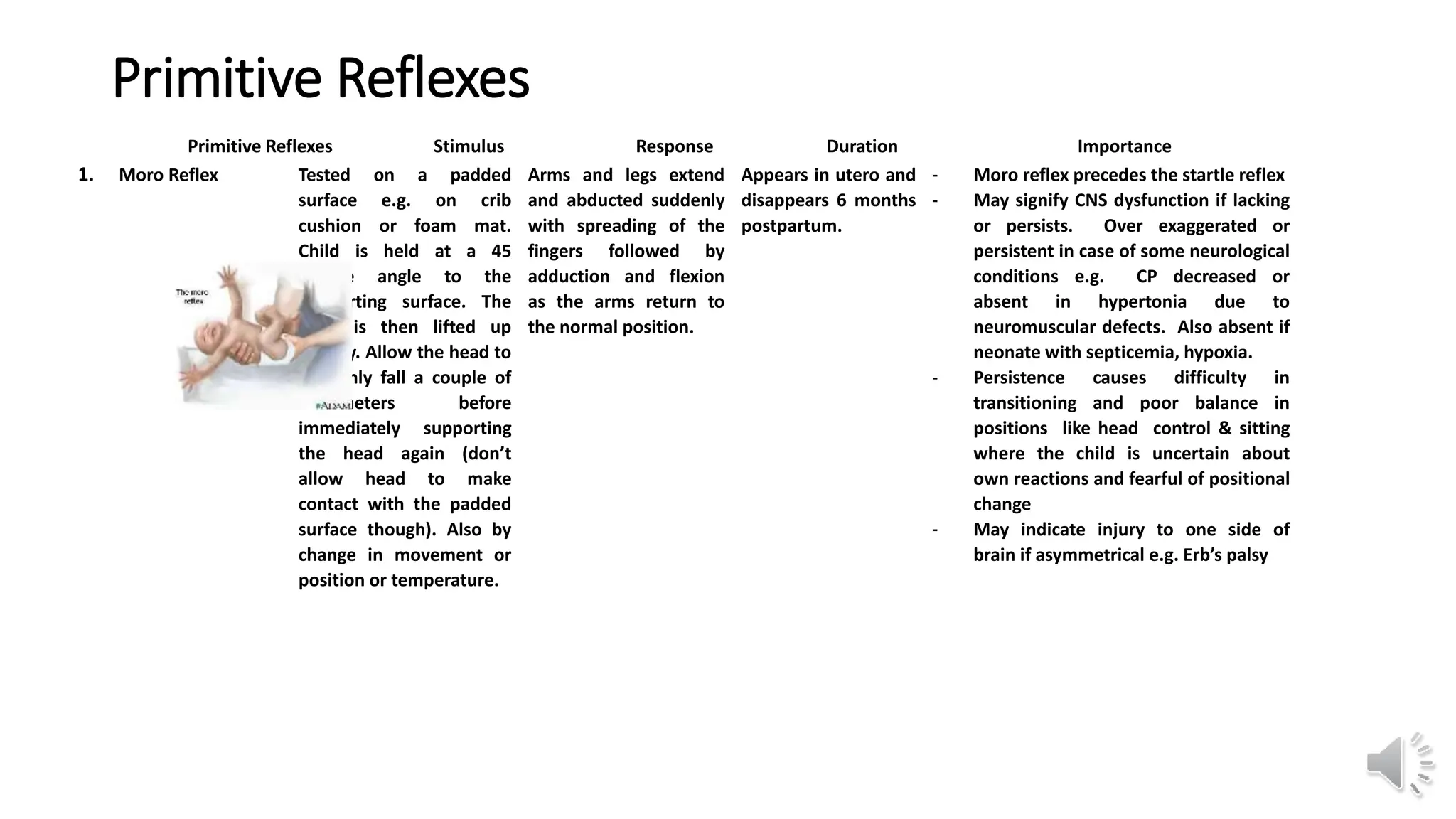
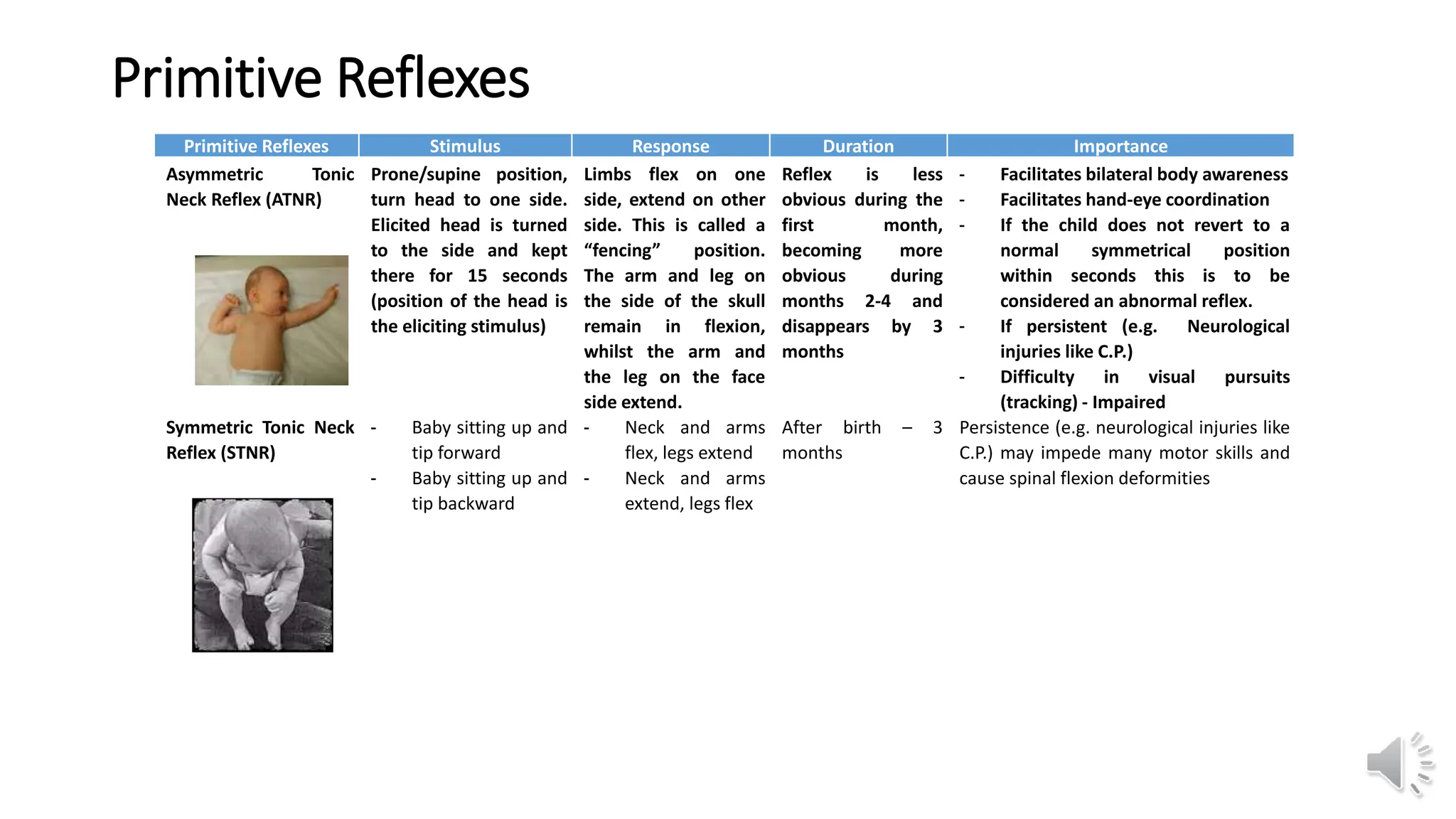
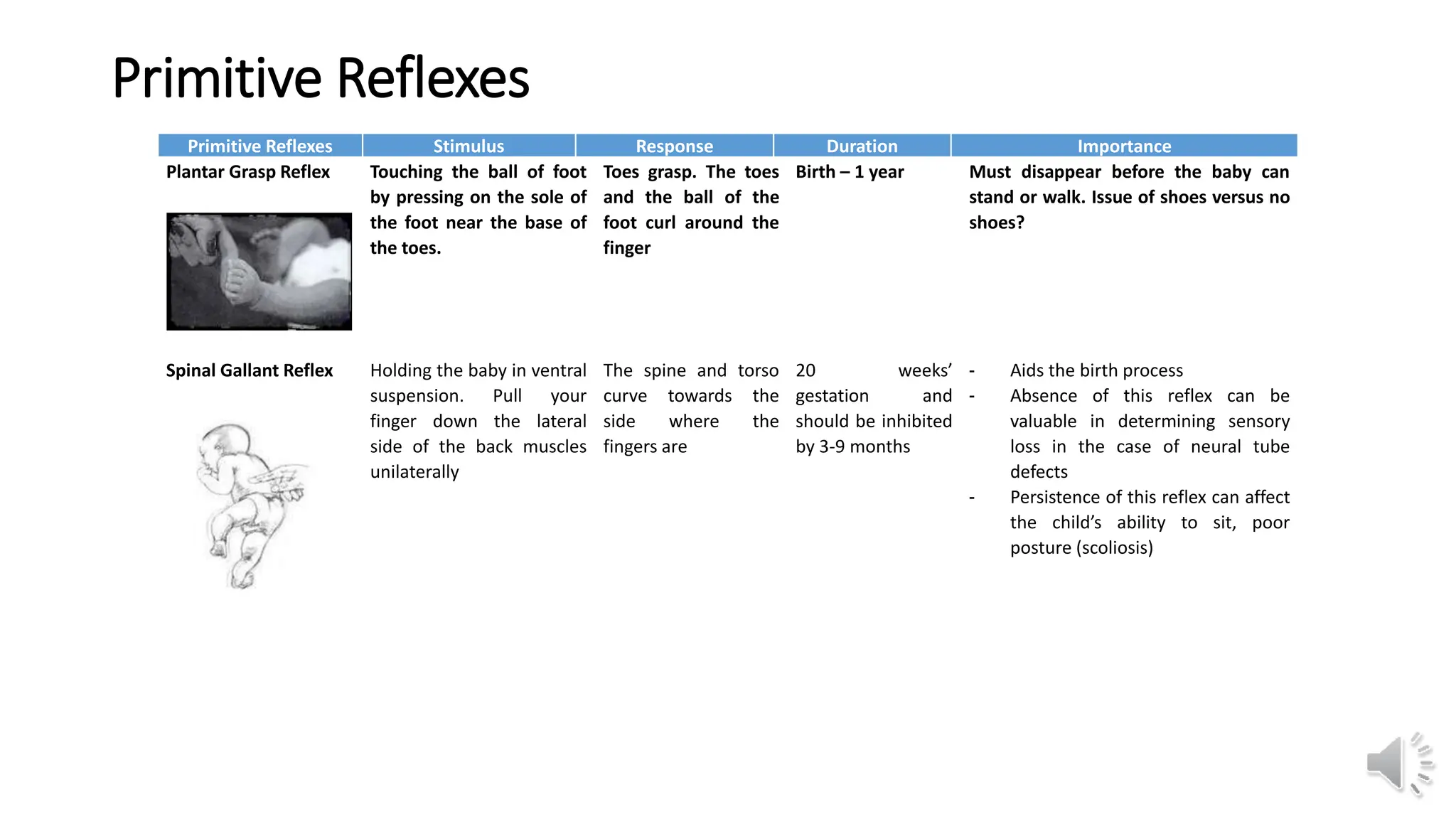
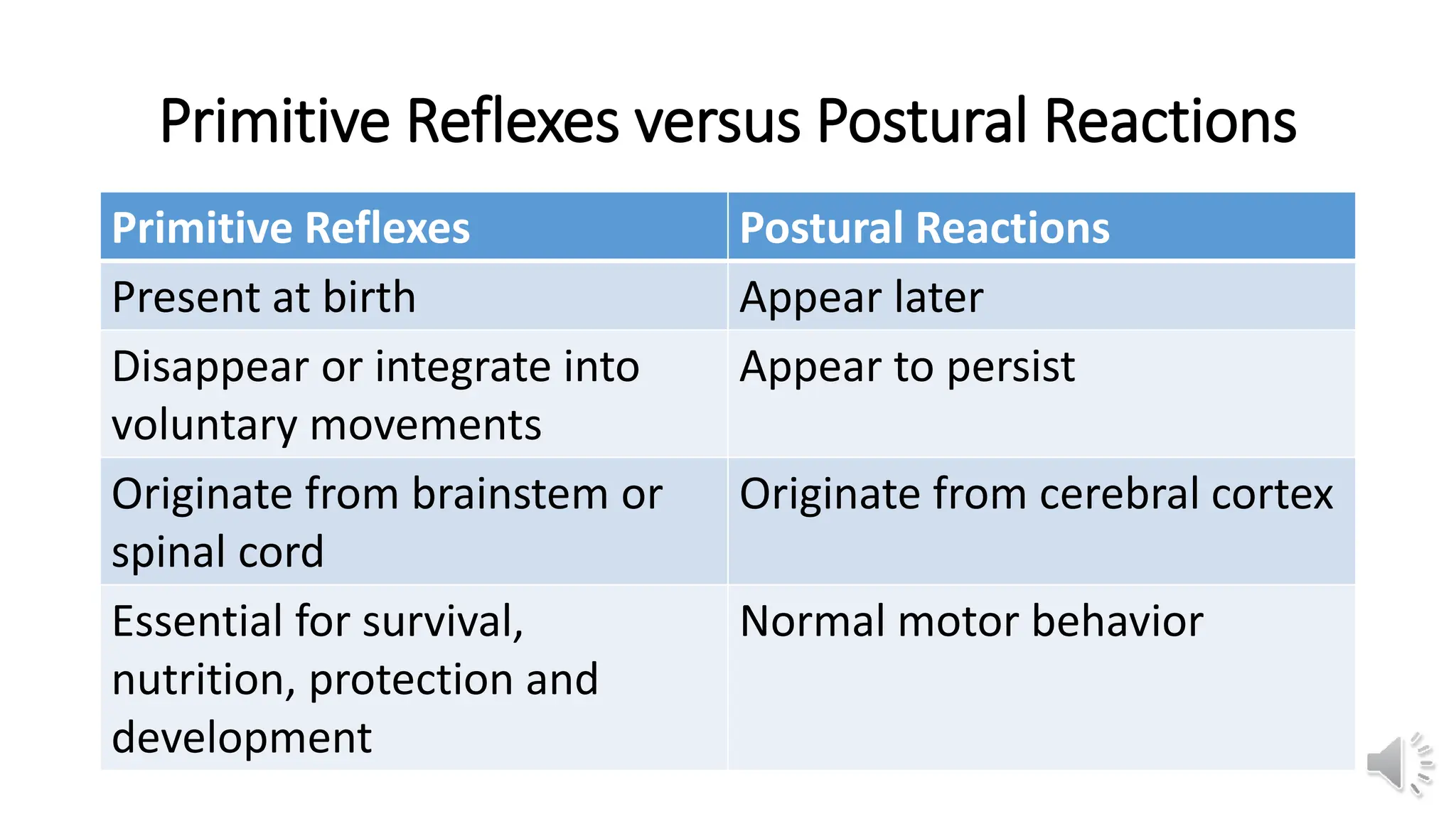
This document provides information about primitive reflexes present in infants at birth. It begins by outlining the learning objectives, which are to familiarize the reader with the primitive reflexes, how to test them, their purpose and development, and the clinical significance of their persistence. It then defines primitive reflexes as involuntary responses originating in the brainstem that are critical for survival in early life. The document lists and describes the most common primitive reflexes, including palmar grasp, rooting, sucking, Moro reflex, and asymmetric tonic neck reflex. It explains that primitive reflexes normally disappear by 6-12 months as voluntary movement develops, and that their persistence may indicate neurological impairment. The document distinguishes primitive reflexes from