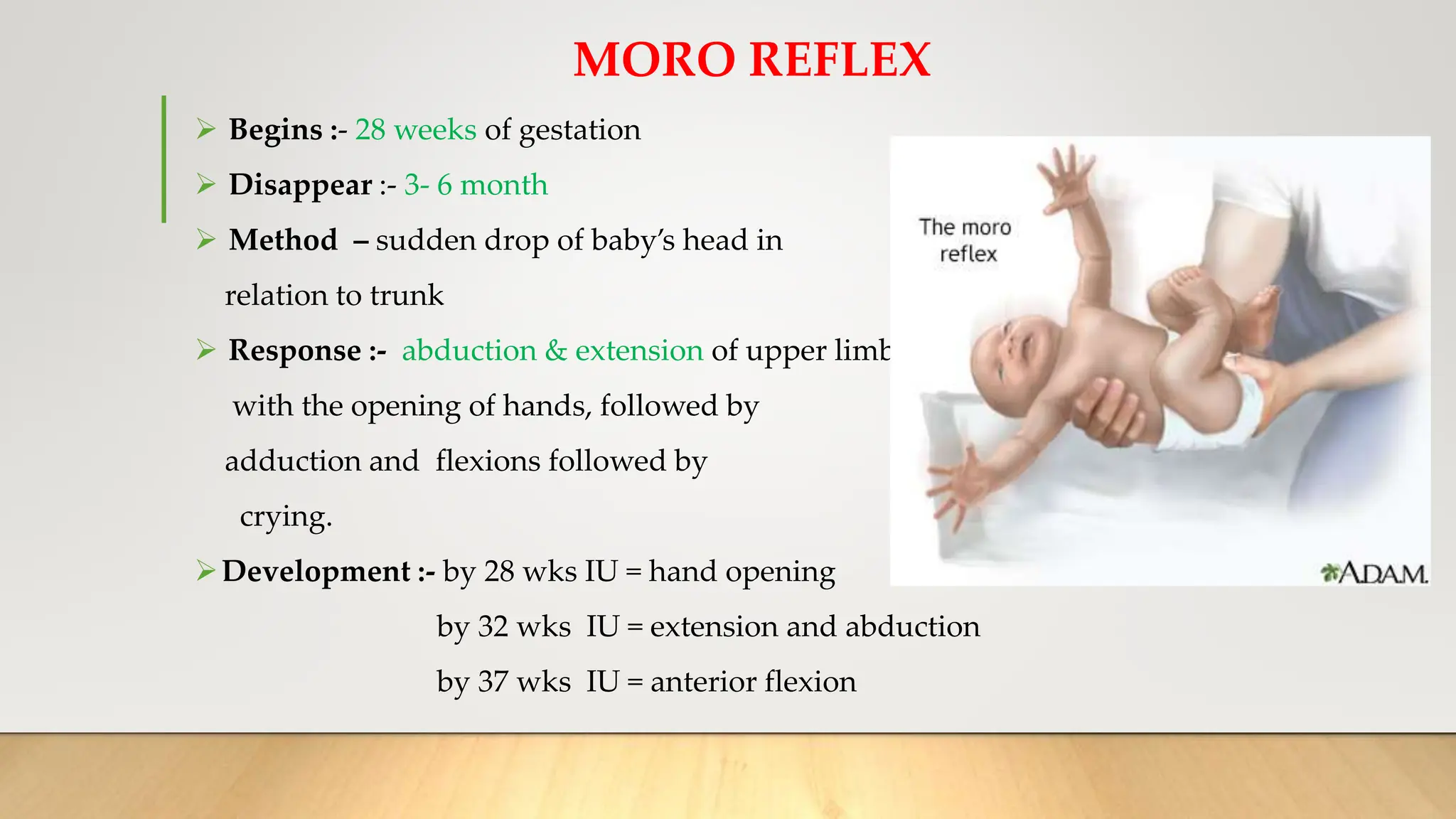
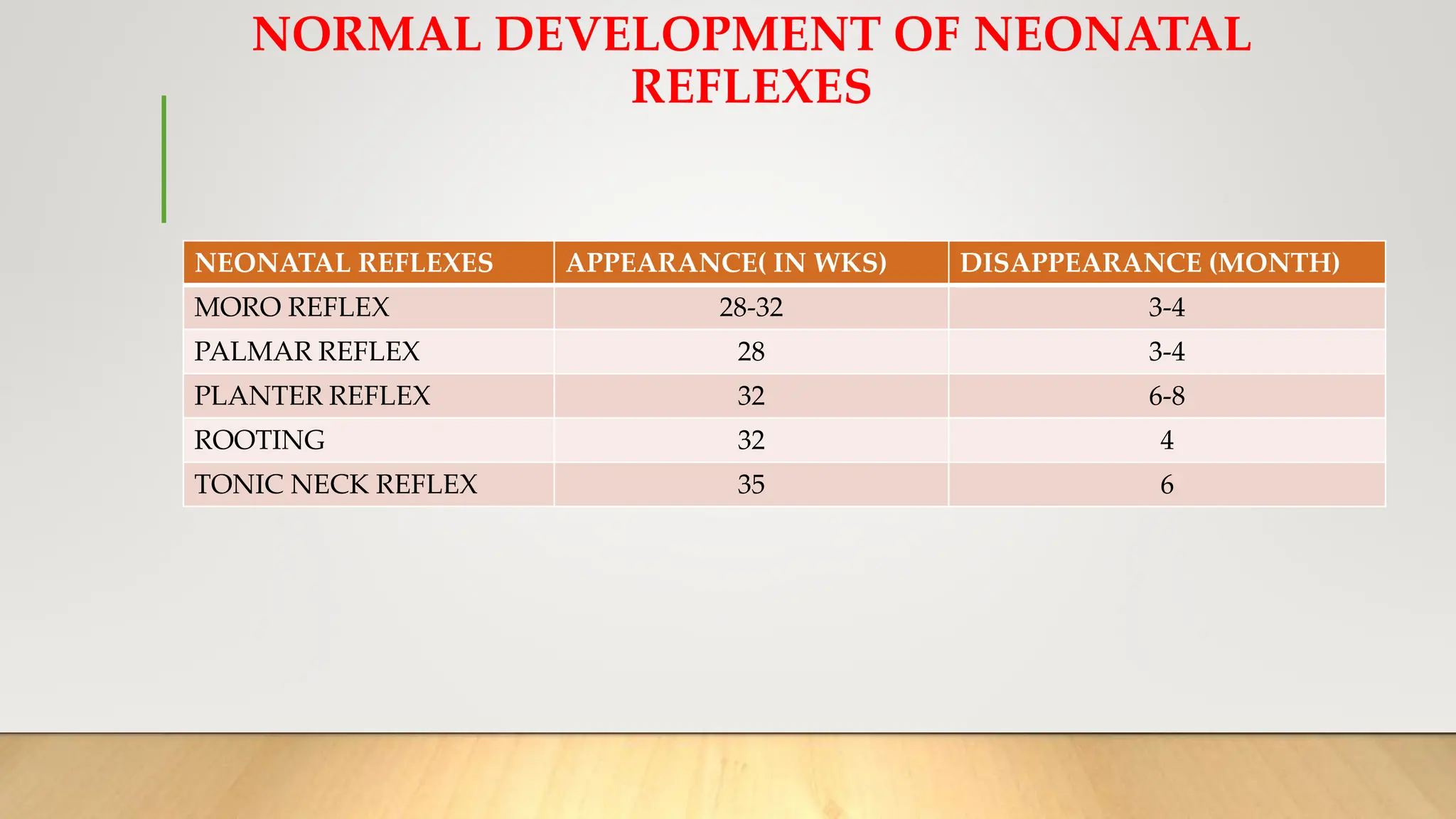
This document discusses newborn reflexes. It defines a reflex as an involuntary action in response to stimulation without awareness. Neonatal or primitive reflexes are inborn patterns that develop in newborns and should be fully present at birth. The document describes several important reflexes like Moro, palmar, plantar, stepping, tonic neck, and oral reflexes. It provides details on when each reflex typically appears and disappears during development. The clinical significance of these reflexes is also explained, such as what abnormalities in the reflexes may indicate.