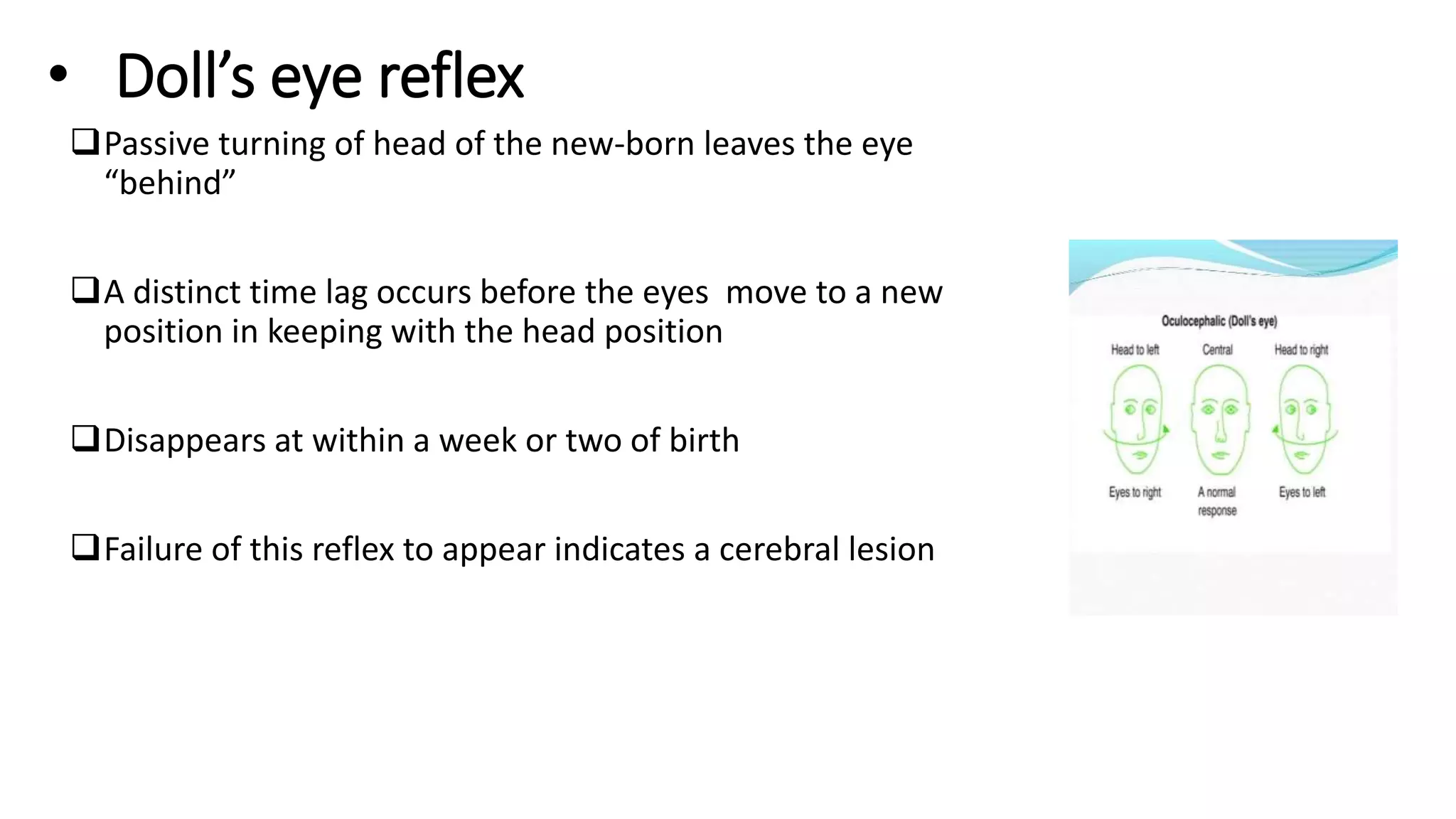
Neonatal reflexes are involuntary responses present at birth that help assess infant development. There are several general body reflexes like the Moro reflex and plantar grasp reflex, as well as facial and oral reflexes. The presence, absence, strength, and timing of reflexes can indicate neurological abnormalities. Understanding neonatal reflexes aids in evaluating whether development is normal or if further assessment is needed.