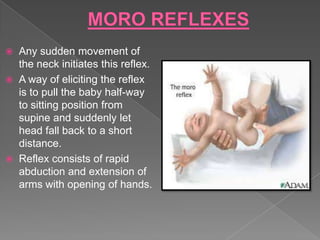
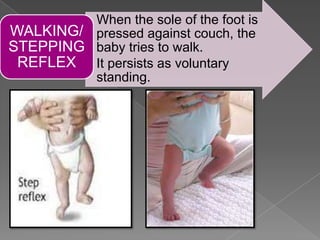
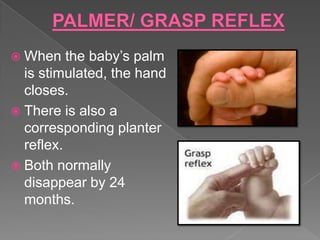
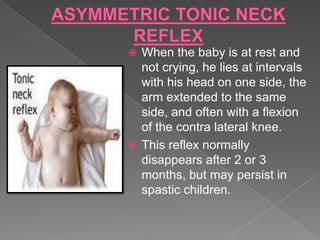
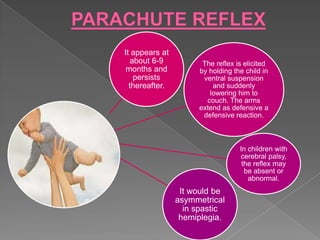
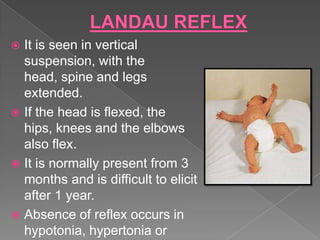
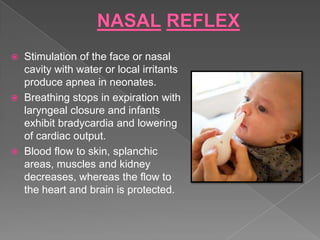
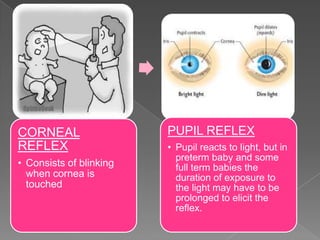
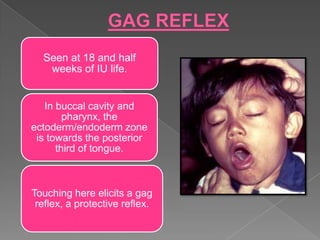
This document summarizes various reflexes present at birth and during early childhood development. It describes general body reflexes like the moro reflex and startle reflex, as well as facial reflexes, oral reflexes, and other reflexes. It provides details on the onset and disappearance of each reflex, how they are elicited, and their significance. The document serves as a reference for understanding reflex development in infants and children.