Downloaded 3,985 times
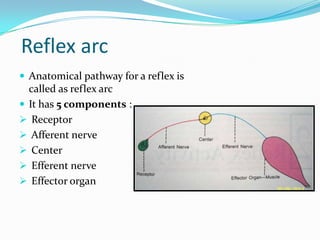

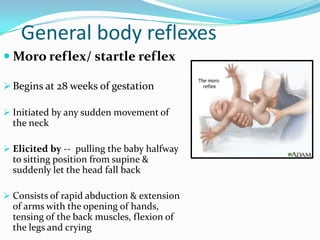
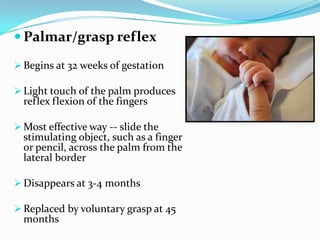
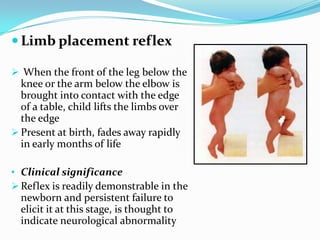
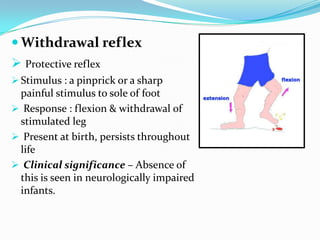
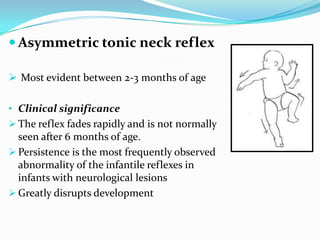
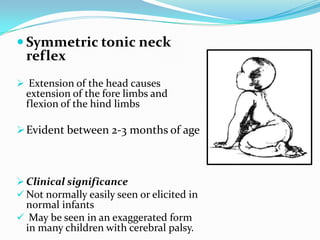
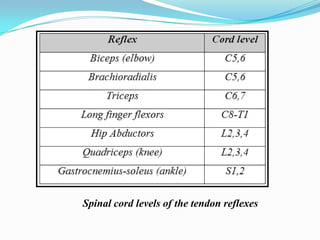


The document discusses various reflexes seen in infants and their significance. It begins by defining a reflex and describing the basic reflex arc involving receptors, afferent nerves, centers, efferent nerves and effectors. Reflexes are then classified based on whether they are inborn or acquired, their neurological pathway, purpose and clinical presentation. Several important reflexes seen in newborns like the moro, rooting and babinski reflexes are explained in detail. The document emphasizes that assessment of infant reflexes helps identify normal development and potential abnormalities.